The Beans or Brain?- The ACORN trial and effects of cefepime and pip-tazo on neuro and renal outcomes
March 4, 2024
In the Emergency Department, we often have to initiate empiric antibiotic treatment for sick, undifferentiated patients. Cefepime and Piperacillin-Tazobactam (pip-tazo) are common antibiotic options for coverage of gram-negative organisms, such as pseudomonas. But is one better than the other? In this podcast, we will critically appraise The ACORN Trial- an article that examines the risks of acute kidney injury and/or neurologic dysfunction in patients treated empirically with one of these antibiotics.
Contributor: Dillon Warr, MD
Effect of Antibiotic Choice On ReNal Outcomes (ACORN)– (PubMed)
The Beans or Brain?- The ACORN trial and effects of cefepime and pip-tazo on neuro and renal outcomes – The SimKit Podcast
Practicing procedures can be tough. Let SimKit do all the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. Get 10% off with coupon code SimKit10
BACKGROUND
Acutely ill adults presenting to the hospital with suspected infection frequently receive empiric antibiotics, and many of these undifferentiated patients receive broad-spectrum antibiotics, such as cefepime or piperacillin-tazobactam as part of their antibiotic regimen.
Cefepime and Pip-Tazo have similar efficacy against gram-negative bacteria, particularly pseudomonas. Our choice to use one of these over the other likely depends on differences in their adverse effect profiles and perhaps a bit on our institution’s culture.
There have been observational studies that have reported an association between Cefepime and neurotoxicity, which can range from agitation all the way to coma.1
There is a better known reported association between pip-tazo and acute kidney injury, particularly with the concurrent receipt of vancomycin.2 There is even a US Food and Drug Administration warning that coadministration of piperacillin-tazobactam with vancomycin may increase the incidence of AKI.3 It is important to note that these previous studies have focused on serum creatinine level as the measure of AKI, rather than patient-centered outcomes such as new dialysis or mortality.
More recently, there have been observational studies noting that the creatinine elevation with Zosyn is a form of pseudo-AKI, ie: the creatinine is briefly elevated due to inhibition of tubular secretion of creatinine, without elevation of kidney injury markers such as cystatin-C.4 These same studies demonstrated that this transient creatinine elevation was not associated with CKD long term or need for hemodialysis.
OBJECTIVE
Determine whether the choice between cefepime and piperacillin-tazobactam affects the risks of acute kidney injury or neurologic dysfunction in patients treated empirically for acute infection with one of these antibiotics.
PROTOCOL
Design
Single center, pragmatic, investigator-initiated, open-label, parallel-group RCT.
Comparison
The safety of cefepime and piperacillin-tazobactam in adult patients with suspected infection in the emergency department or medical intensive care unit.
Inclusion Criteria
Adults ≥18 years of age in the ED or medical ICU for whom a clinician initiated an order for cefepime or pip-tazo within 12 hours of presentation to the hospital.
Exclusion Criteria
- Allergy to cephalosporins or penicillins
- Received more than 1 dose of an antipseudomonal cephalosporin or penicillin within the previous 7 days
- Incarcerated
- If the treating clinician determined that 1 of the two drugs represented a better treatment option for that patient.
Methods
- An EMR tool screened all patients for eligibility and an automated alert within the EMR prompted doctors to consider enrolling the patient in this trial. The EMR was programmed to automatically screen the patient for exclusion criteria. If none were found, their antibiotic order triggered a prompt for the doctor to consider enrolling the patient in the trial.
- Informed consent was also waived as the study was deemed minimal risk, both antibiotics are considered standard of care, and this was considered an emergency intervention given they were acutely ill and hospitalized.
- Patients were then assigned via simple randomization without stratification in a 1:1 ratio to receive cefepime or piperacillin-tazobactam. Group assignment was concealed until enrollment.
- The dose and frequency of antibiotic was determined by institutional protocols.
- Cefepime: 2-g intravenous push over 5 minutes every 8 hours
- Pip/Tazo: 3.375-g initial bolus over 30 minutes, followed by an extended infusion of 3.375 g every 8 hours infused over 4 hours for subsequent doses.
- The duration of antipseudomonal treatment was determined by the treating clinician.
- The clinicians also were free to administer additional non-psuedomonal antibiotics, such as vancomycin and metronidazole, based on their own clinical judgment.
- If treating clinicians tried to change or discontinue the assigned antibiotic in the 7 days following enrollment, the EMR automatically reminded them of the ongoing trial and recorded the reason for cessation or the change.
Primary Outcome
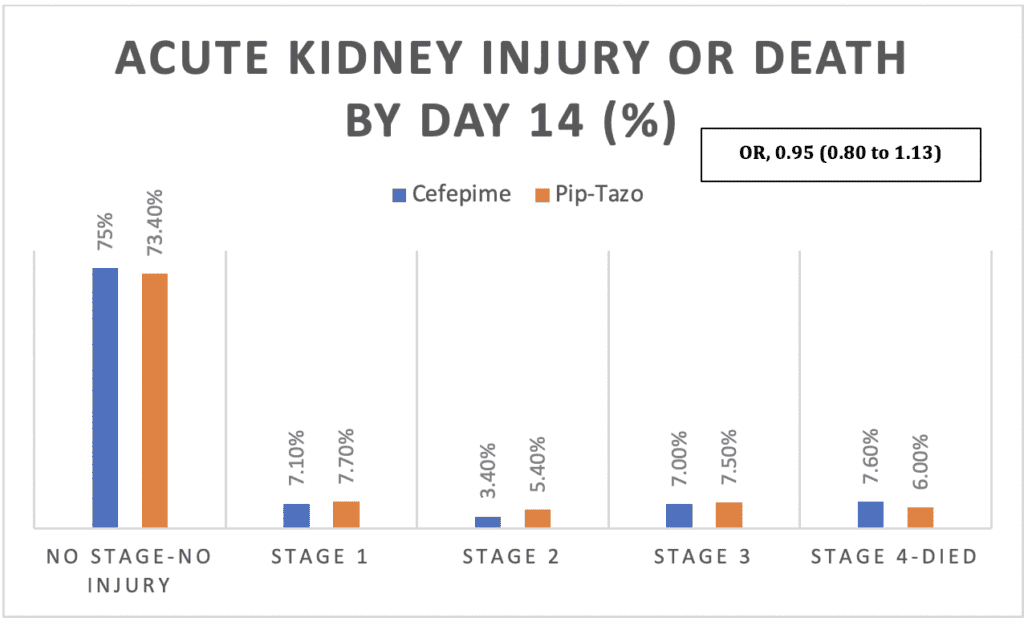
Highest stage of AKI or death arising between randomization and day 14, measured on a 5-level ordinal scale.
- Score 0: Did not experience new or worsening AKI were assigned a value of 0.
- Score 1-2: Mild and Moderate AKIs.
- Score 3: Really bad AKIs or needing hemodialysis were assigned a value of 3.
- Score 4: They died during study period.
Baseline creatinine levels were taken during the year before hospitalization if possible. If not, baseline was the lowest level since trial enrollment.
Secondary Outcomes
Two secondary outcomes were prespecified.
- The proportion of patients who experienced a major adverse kidney event at day 14 or at hospital discharge (whichever occurred first), which was a composite of death, receipt of new HD, or persistent kidney dysfunction, defined by the final inpatient creatinine being >2 times the baseline level.
- The number of days alive and free of delirium and coma within 14 days, which was the number of calendar days on which the patient was alive and without a positive CAM-ICU or RASS score of -4 or -5, at time of hospital discharge.
Statistical Analysis
They predicted that enrolling 2500 patients would provide 92% power for detecting an odds ratio of 0.75 in the primary analysis, or an absolute between-group difference of 5% in patients who experienced AKI of any stage or death.
Data were analyzed by intention to treat analysis both using unadjusted and adjusted models. They also had several other prespecified sensitivity analyses and prespecified analyses on the effects of baseline patient variables.
RESULTS
Population
Among 3806 patients who met inclusion criteria:
- 30.8% were excluded.
- 95% were included in the primary analysis after excluding those who never received a study drug after enrollment.
- 2511 patients were included in the primary analysis, meeting their prespecified 92% power threshold.
Characteristics
- The median age was 58
- Roughly 57% male
- 77% non-Hispanic white.
- 94.7% of patients were enrolled in the ED.
- The median time between presentation to the hospital and enrollment was 1.2 hours.
- 54% had sepsis at enrollment, with the most common sources of infection being intra-abdominal and pulmonary.
- The median SOFA score was 2.
- 48.3% of the patients were assigned to the cefepime group and 51.7% to the Pip-Tazo group.
- Other baseline patient characteristics, including initial AKI stages, creatinine, and RASS, were well-balanced.
Antibiotic Therapy
In the 14 days after enrollment:
- 95% in the cefepime group received at least 1 dose of cefepime.
- 98.4% in the pip-tazo group received at least 1 dose of pip-tazo.
- Patients in each group were treated for a median of 3 days.
- ~18% in each group receiving at least 1 dose of the other antibiotic.
- 77% of patients in each group were receiving IV vancomycin at the time of enrollment, with a median duration of vancomycin treatment of 2 days.
Primary Outcome
The highest stage of AKI or death by day 14 did NOT significantly differ between cefepime and Pip-Tazo, (OR 0.95, 95% CI, 0.80-1.13). 75% in the cefepime group and 73% in the Pip-Tazo group did NOT experience AKI of any stage or death by day 14. These results were similar in the adjusted analysis and in all pre-specified analyses, including the intention-to-treat population.
Secondary Outcomes
- There was no significant difference between groups experiencing a major adverse kidney event at day 14 (10.2% in the cefepime group, 8.8% in the Pip-Tazo group).
- By day 14, 3.3% in the cefepime group initiated hemodialysis while 2.3% of the patients did in the Pip-Tazo group.
- Patients in the cefepime group experienced significantly fewer days alive and free of delirium and coma within 14 days compared with patients in the pip-tazo group (11.9 days vs 12.2 days; AD 0.3 days). (OR, 0.79 [95% CI, 0.65 to 0.95]).
- Significant difference between the cefepime group and pip-tazo group when it came to coma or delirium. 20.8% of the cefepime group experienced coma or delirium between enrollment and day 14 compared with 17.3% in the pip-tazo group. (AD, 3.4% [ 95% CI, 0.3%-6.6%].

STRENGTHS- excellently designed clinical trial.
- The ACORN trial tried to answer an important clinical question with true equipoise: “Cefepime or pip-tazo, which is better?”.
- They used primary and secondary endpoints that people care about, particularly how the choice between antibiotics affects the risks of acute kidney injury or neurologic dysfunction.
- They had simple inclusion and exclusion criteria–basically was this an adult patient in the ED or ICU who is sick and a clinician plans to start one of these antibiotics.
- They also had an amazing method of enrolling patients, levying the EMR and everyone’s favorite BPA notifications. As a result, they were able to enroll over 2600 patients at a single center in only 1 year.
- Randomized control trial with strong internal validity with effective randomization
- Well balanced baseline characteristics.
- Majority receiving intervention as randomized.
- It met its sample size for 92% power.
- It conducted prespecified sensitivity analyses and analyzed both adjusted and unadjusted data by intention-to-treat.
LIMITATIONS
- It was a single academic center which could limit generalizability.
- Approximately 20% of patients received the alternative antibiotic, which could bias towards the null (though exposure was similar in both groups).
- The median duration of antibiotic exposure was short (~3 days), though this reflects common practice at hospitals when it comes to many undifferentiated ED patients. Patients get started on Abx and get narrowed or have Abx discontinued once cultures result. It makes it challenging, however, to extrapolate to prolonged courses of these antibiotics.
- Only about 50% of patients were found to have sepsis on retrospective assessment and many were not that sick based on SOFA scores at time of enrollment
- The dosing regimen may not reflect dosing in other parts of the country.
- Rapid dose IV push cefepime as performed in this study in some studies has been associated with enhanced toxic effects.
- The primary outcome, AKI stage, is not a true patient centered outcome. However, they did include hemodialysis and death as part of their ordinal scale and as part of a composite secondary outcome. In addition, given that the clinical conundrum for physicians is concern about Pip-Tazo +/- Vanc and renal impairment, this AKI stage does have some clinical decision making relevance. If anything, the data lends further support to the notion that even in those patients with a transient rise in creatinine, there is no meaningful “patient-centered” bad outcome for the use of Pip-Tazo.
- Although they had a large sample size for a single center site, one has to be careful with secondary outcome measurements even with significance, such as the higher rates of neurologic dysfunction seen in the cefepime group in this study.
- The biggest limitation is the unblinded nature of the study. While it may not significantly impact objective data like creatinine measurements, it definitely can introduce bias into the assessment of neurologic dysfunction.
- Clinicians may have been more likely to make the diagnosis of encephalopathy with cefepime using the CAM-ICU or RASS assessments, especially as these assessments are subjective in nature themselves.
- Given that this secondary outcome was only just shy of insignificant, caution must be had when applying these data to clinical practice.
- Anyway, is a between-group difference of 0.3 days alive and free of delirium and coma within 14 days clinically significant?
AUTHORS CONCLUSIONS
“Among hospitalized adults in this randomized clinical trial, treatment with piperacillin-tazobactam did not increase the incidence of AKI or death. Treatment with cefepime resulted in more neurological dysfunction.”
OUR CONCLUSIONS
Ultimately, despite these limitations mentioned above, The ACORN trial demonstrate that piperacillin-tazobactam does not increase the risk of AKI compared with cefepime. At least based on this study and short term exposure, we can put to bed this pip-tazo/vancomycin nephrotoxicity concept that has plagued ED physicians–especially with the supporting evidence from previous observational studies showing the pseudo-AKI nature of the vancomycin-Zosyn combination.
While we cannot make a strong case for avoiding cefepime because of its potential to induce neurologic dysfunction based on this study, this study is a good reminder to be aware of this possible adverse effect and keep it on your differential for causes of ICU delirium.
In my practice, unless there is a specific clinical indication to use cefepime, I will continue to use pip-tazo first for undifferentiated patients with sepsis or possible sepsis. An argument for a different day is whether or not we actually need anti-pseudomonal coverage for community acquired infections or sepsis in the first place.
READ MORE ABOUT IT
NEJM Journal Watch: https://blogs.jwatch.org/hiv-id-observations/index.php/a-brilliant-strategy-for-conducting-clinical-trials-the-acorn-study/2023/10/17/
THEBOTTOMLINE: https://www.thebottomline.org.uk/summaries/icm/acorn/
RESOURCES
- Appa AA, Jain R, Rakita RM, Hakimian S, Pottinger PS. Characterizing cefepime neurotoxicity: a systematic review. Open Forum Infect Dis. 2017;4(4):ofx170. doi:10.1093/ofid/ofx170 (PubMed)
- Bellos I, Karageorgiou V, Pergialiotis V, Perrea DN. Acute kidney injury following the concurrent administration of antipseudomonal β-lactams and vancomycin: a network meta-analysis. Clin Microbiol Infect. 2020;26(6):696-705. doi:10.1016/j.cmi.2020.03.019 (PubMed)
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/050684s88s89s90_050750s37s38s39lbl.pdf
- Miano TA, Hennessy S, Yang W, et al. Association of vancomycin plus piperacillin-tazobactam with early changes in creatinine versus cystatin C in critically ill adults: a prospective cohort study. Intensive Care Med. 2022;48(9):1144-1155. doi:10.1007/s00134-022-06811-0 (PubMed)


