The Awake Shoulder Reduction- the way of the future
February 16, 2024
Anterior shoulder dislocations are common in the Emergency Department and let’s face it, fun to fix. But this can be a time and resource intensive endeavor- especially if doing IV sedation. In this podcast we look at intraarticular analgesia as an alternative to IV sedation to allow for an awake shoulder reduction. And we show you several examples of how successful this can be!
The Awake Shoulder Reduction- the way of the future – The SimKit Podcast
Transcript
Hello, hello, hello Everyone and welcome to the SIM Kit podcast and we’re going to talk today about one of my favorite things to do as an emergency medicine clinician and one of my favorite things to talk about reducing shoulders in the emergency department. Now reducing shoulders in the ED is about as common as a Turkey sandwich. The shoulder is the most commonly dislocated joint, requiring reduction and 95% of these are going to be anterior shoulder dislocations. Now, no matter where you work, reducing these shoulders can be very time and resource intensive endeavors, but they do not have to be. In the old days, this required sedation with IV medications, which entail having a nurse, a respiratory therapist, ideally a physician controlling the sedation, and a physician doing the reduction. With ED overcrowding and bed availability issues, reducing these shoulders can often be delayed. While these resources are being obtained or procured for completing the reduction. And we know that the longer the shoulder is out, the more spasm the patient experiences and the more difficult the reduction can be. So in this podcast, we want to talk about two elements of reducing anterior shoulder dislocation. Options. We’re going to talk about IV sedation versus intraarticular anesthetics and useful reduction techniques. The goal here is to outline an approach that allows for a single provider plus a non medical assistance such as a tech to reduce the shoulder with minimal pain to the patient’s lower risk for adverse events related to procedural sedation. And shorter length of stay for the patient in my opinion, after the review of this literature, this is the approach we should all be taking in the emergency department. Now let’s dive into the Intraarticular block and its comparison to IV sedation. There have been several randomized controlled trials comparing these two. From this, there have been at least three systematic reviews and meta analysis. Now I mentioned that there are several men announces out there, but we are going to be focusing on the most recently published one and the others will be LinkedIn, the show notes. This was published in April 2022 in the Canadian Journal of Emergency Medicine and directly compares Intraarticular Lidocaine versus IV sedation for acute anterior shoulder dislocation in the emergency department. Exactly what we’re talking about here. So this meta analysis found 12 randomized control trials, including 630 total patients comparing intraarticular, lidocaine and 327 patients versus investigation and 303. The paper did a nice job scouring the world’s literature out there, started out with many, many studies, and their systematic review ended up including the 12 randomized controlled trials. In their comparison, they looked at Ed length of stay pain scores after the anesthetic and before the reduction. The reduction, pain score, procedural success and procedure. Super, super importantly, when we are looking at outcomes like this, we need to see what we’re comparing table one in the article shows the medications used and intraarticular lidocaine either 20ML’s or 4 milligrams per kilogram were used for the intraarticular element. Now, there were a variety of different IV medications used, including the following. Demerol and Valium. Propofol alone or in combination with fentanyl and ketamine. Midazolam and fentanyl. Propofol or etomidate, morphine and diazepam, and morphine and midazolam. Now I want to pause here just for a moment and talk about what might be appropriate sedation in these cases. In the modern era, the most commonly used medications for sedation include probably propofol, cardamine, and possibly etomidate. I know I’m using that for my cardioversions. When comparing these agents and thinking about overcoming muscle tonicity, ketamine and automate seem like less ideal options because of the maintained tone with ketamine and the potential for myoclonus with etomidate and is very short duration of action. This leaves propofol as probably the ideal agent for these circumstances because of the muscle relaxation. This of course, has to be weighed against apnea aspiration and hypertension as adverse events. So coming back to our article, what did they find? And in looking at the most important outcome probably from our perspective, successful reduction, they found no difference in reduction success between intraarticular lidocaine and IV. They did find that reduction success was 83.8 in the Intraarticular Lidocaine group versus 91.4 in the procedural sedation. So different numbers there, but not statistically significant. Now the meta analysis included 12 studies, six of which were rather old and used medication combinations that are not commonly used any longer. Now they did a subgroup analysis, looking at the six studies that excluded the older medications used for IV sedation. Which did not change the results of comparable reduction success. But noted that the Intraarticular had a 83.8% success rate versus IV sedation now at 95.7. A definitely notable difference in success rate, but not statistically significant. Now this difference in success rate has to be weighed against adverse events, right? What did they find in this study? There were statistically significant differences in adverse events rates with fewer occurring in the Intraarticular Lidocaine Group, 1.3 versus 20.8. Sent pretty massive difference here as we all know the complications of IV sedation are not trivial, including hypoxia which depending on severity may be minimal, prolonged sedation, hypotension, vomiting, among others. How about length of stay? They found that seven studies with 299 patients. Reporting on length of stay, the data shows a statistically significant difference in length of stay paving intraarticular lidocaine with an average difference of 1.48 hours. That’s right, shorter length of stay by 1.48 hours for the intraarticular lidocaine group. For pain scores, they saw no difference after administration of analgesia before the reduction or change in pain score. In the pre anesthesia to post reduction time frame. The procedural time was longer in the Intraarticular Lidocaine group with a difference of eight minutes. Ease of reduction was not statistically different between the groups. What about patient satisfaction? This is an interesting one. In the six studies assessing this with 380 patients, there was a significant difference with decreased patient satisfaction in the intraarticular lidocaine group. We’ll definitely talk more about this in our discussion. The authors also did a cost analysis of this, which of course showed markedly lower cost in the patients getting intraarticular lidocaine. Much lower resource utilization. The authors appropriately conclude that intraarticular decline may have similar effectiveness as IV sedation and successful reduction of the anterior shoulder dislocation with fewer adverse events, shorter length of stay, and no difference in pain scores or ease of reduction. Patient satisfaction was notably lower in the intraarticular lidocaine. Group. So what are our take, homes? What do we think about this study and this data? This is the most current, most up-to-date literature comparing intraarticular anesthetics to IV sedation. It is worth noting that Lidocaine was by far the most commonly used intraarticular agent, but there is an ASAP managing acute pain in the emergency department about using intraarticular injections into the shoulder and they note that you can use bupivacaine ropivacaine or lidocaine. So I believe there’s a dealers choice element there. But note that this article is comparing lidocaine to other agents. This article is also important in that it includes some new studies which more accurately represent the current IV sedation medications being used. I think this is pretty strong evidence showing equipose or nearly equipose with the two techniques. Certainly in terms of the reduction success and decrease in pain scores for the patients, it is definitely worth noting that success rate was not the same. It was not statistically different, but 83.8 versus 95.7 when comparing. Current IV sedation medicines that 12% difference is worth being noted that of course of course has to be weighed against our adverse event rates, which was about a 20% change in the intraarticular group versus the IV Sedation group. And then time, time is something invaluable to an emergency department, to a provider, to patient and a 1.5 hour length of state difference is not something to sneeze at and is very important when we’re considering what agents to use here. So I think you are well supported by the literature. If you want to use the intraarticular approach. And of course this is my preferred method. Now let’s move topics here and talk about our reduction techniques. Which technique is best for reducing an anterior showed dislocation? Amazingly, there are over 20. That’s right, 20 different reduction techniques that have been described, and many of these are eponyms associated, which makes them really pretty hard to remember. They can, however, be broken down into 3 relative categories. These include rotation and leverage, muscle balance and relaxation and traction. Looking at common techniques in each category, rotation and leverage includes the Kocher method, external rotation, and Spazzo muscle balance and relaxation includes Fares Milch, Cunningham, and Simpson and Traction includes the old Hippocratic way of the foot in the axilla and pulling really hard traction counter traction and Davos. Now an article was published in Annals Emergency Medicine 2023 that is a meta analysis comparing these techniques. The reference is in the show notes. In this article, which included fourteen studies and almost 1200 patients, Davos and Fares had the most favorable success rates, Fares and modified external rotation had the most favorable reduction times and Fares had the most favorable pain scores during reduction, now it should be recognized that this is a very very heavily statistical analysis type study. It is rather difficult to interpret as a non statistician. The study is comparing procedure types and relies obviously on the 14 studies that went into it. Diving into that more, we see that only one of the 14 had the Cunningham included in the comparison and it was excluded in many of the analysis because of the lack of IV sedation. This study is worth noting for completeness sake, but given the limitations of literature out there, should not be considered a definitive assessment of the many reduction techniques, and there’s definitely an apples to oranges comparison element to this. That said, it is worth noting that the Fares technique did shine in this article. Again, being favorable for success rate for reduction time and for pain scores, the Davos and the modified external rotation technique are also worth mentioning here.
OK, now with all of this data, what is the best approach? What do I do and what do we recommend? I think the preponderance of data shows favorable outcomes and really significant decreased length of stay when using intraarticular injection. This is my personal practice. I diagnose the anterior shoulder dislocation clinically by appearance. If there’s any suspicion, or if the patient’s habitus necessitates it, I get an X-ray to confirm. I then use bupivacaine .5 per cent. I inject 10 mils using the posterior approach. Remember that with these anterior dislocations, the joint space is wide open and this is a very, very easy hit to get intraarticular and aesthetic. I like to try to do this as early as possible to give the medication some time to marinate before attempting the reduction. I will sometimes add an oral or intranasal benzodiazepine to help with anxiety and muscle relaxation, depending of course on the patient during this whole process, and particularly during the reduction attention to patient anxiety. And keeping them informed is paramount. As noted in the meta analysis, patient satisfaction can be reduced and there can be some anxiety about remaining awake during the reduction. I use my most calm voice and highlight high degrees of experience and confidence in this. I’ve had patients where upon me entering the room, they immediately tell me that I have to call ortho and prep the OR be successfully reduced awake with an intraarticular block by talking them through the procedure, assuring them there will be no surprises or sudden movements. And getting us to work as a therapeutic team. Once the enter articular block has time to work, I then grab an available tech and work with them on my Cunningham technique. During this they are massaging the deltoid, trapezius and most importantly, the bicep, which can create a bow string effect when in spasm to relax the musculature. I keep the patient adducted against the body with the elbow flexed to 90° and provide gentle downward traction while the massage is happening. During this and in conversation with the patient about us as a therapeutic team, I have two requests of the patient. I asked them to make their body fully like Jello, except for one important exception to stick out their chest like Superman, and pretend they’re pinching a pencil between their shoulder blades. After about 5 minutes of massage and downward traction, if not successful, I inform the patient about and do a slight external rotation, bringing the forearm out away from the body. Sometimes a very small amount of pressure on the human head will also facilitate the reduction. This is almost universally successful. If not in light of the literature we just discussed, I try a fairs reduction technique. If the patient is agreeable. In the one instance I have not had success here. I put the patient in Davos position with Coban to the wrists and they reduced. Of course, there are some patients that, no matter how calm you are in their presence, how effective your Jedi mind tricks are to help relax them and gain their confidence. They cannot tolerate an awake reduction technique. In these cases, it is of course OK to proceed to IV sedation. So in summary, we recognize that anterior shoulder dislocations in the emergency department is very common. And successfully reducing them can be a time and resource intensive endeavor, especially when using IV sedation. There’s support in the literature for using intraarticular and aesthetic as an alternative if following the literature best practices there, your agent would be lidocaine, but note that bupivacaine and ropivacaine. Are acceptable alternatives as outlined by ACEP. The data shows that using an intraarticular block has a greater than 80% success rate for getting reduction with much lower length of stay and adverse events for the patient. We have to be conscious of patient satisfaction and can improve that by being calm, confident and keeping the patient informed. In terms of reduction technique, note that that we are a little limited in the data that’s out there and creating an apples to apples comparison, but note that that 2023 meta analysis showed favorable characteristics for the fares, modified external rotation, and the Davos techniques. It is my personal practice to get a intraarticular block in early on a patient with an anterior shoulder dislocation and use a tech to assist me in doing a Cunningham technique. This has proven to be very successful and we have several video demonstrations of actual patients where we’ve done this technique included in the show notes, which are definitely definitely worth a watch. So I hope this review of the literature has helped inform your approach to the anterior shoulder dislocation to help improve or maintain your success, decrease your length of stay, decrease your patient adverse events, and maintain patient satisfaction by showing them just how boss you can be with an awake reduction. Thanks for listening.
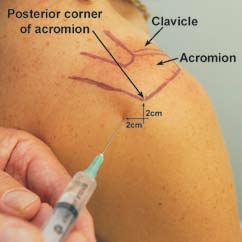
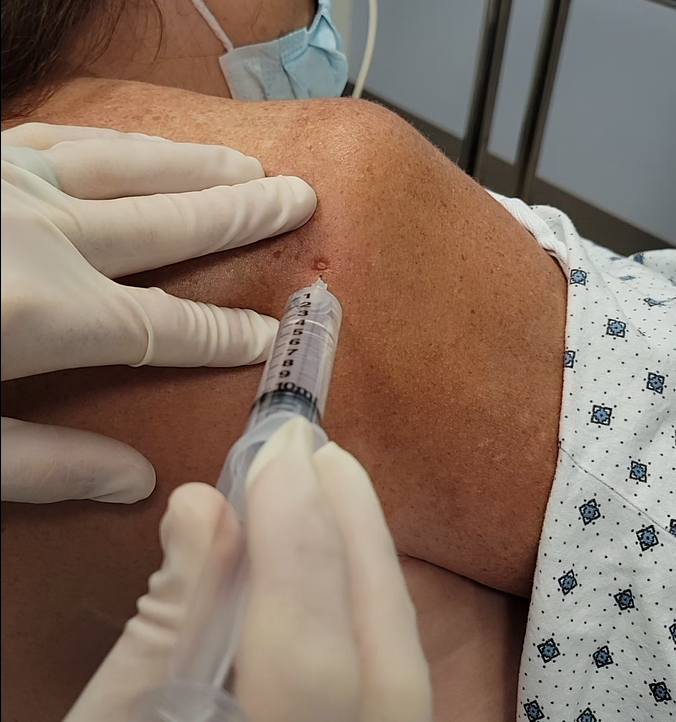
Posterior Intraarticular Injection
Injecting the shoulder with the posterior approach is suuuuuper easy when the humeral head is dislocated anteriorly. Simply find the posterior corner of the acromion, go 2 cm inferior and 2 cm medial, aiming for the coracoid process with your needle insertion. Prep the skin with chlorhexidine or other antiseptic, and inject your anesthetic after introducing your needle 1-1.5 cm (on the average sized patient). Below we show a demonstration image and an injection in an actual patient
Examples of Awake Cunningham Reductions
Patient 1*
Patient 2*
*written consent obtained for all patient cases and best effort to conceal patient identity was used.
Summary
Anterior shoulder dislocations are common in the ED and can be time and resource intensive to reduce, especially when doing sedation. The data supports an intraarticular block as a viable alterative to full sedation with similar (though not identical) success rates, shorter length of stay, lower adverse event rates, and less cost. Patient satisfaction must be a focus when doing an awake reduction, and patient coaching and preparation are paramount.
The literature on reduction technique is sparse and problematic, with the reviewed meta-analysis discussed suffering from an apple-to-oranges phenomenon. That said, the Fares, Davos, and modified external rotation techniques do show a signal toward superiority.
It is my personal practice to get an intraarticular block in early, thorough coach and prep the patient on the approach, and grab a tech for a Cunningham technique. The data shows this to be 80+% successful, which is fantastic. That said there are just some patients where sedation and reduction will be necessary.
Practicing procedures can be tough. Let SimKit do all the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. We want you to be confident and competent clinicians, and we have the tools to help.
References
- Fitch RW, Kuhn JE. Intraarticular lidocaine versus intravenous procedural sedation with narcotics and benzodiazepines for reduction of the dislocated shoulder: a systematic review. Acad Emerg Med. 2008 Aug;15(8):703-8. [pubmed]
- Jiang N, Hu YJ, Zhang KR, Zhang S, Bin Y. Intra-articular lidocaine versus intravenous analgesia and sedation for manual closed reduction of acute anterior shoulder dislocation: an updated meta-analysis. J Clin Anesth. 2014 Aug;26(5):350-9. [pubmed]
- Sithamparapillai A, Grewal K, Thompson C, Walsh C, McLeod S. Intra-articular lidocaine versus intravenous sedation for closed reduction of acute anterior shoulder dislocation in the emergency department: a systematic review and meta-analysis. CJEM. 2022 Dec;24(8):809-819. [pubmed]
- Gonai S, Yoneoka D, Miyoshi T, da Silva Lopes K. A Systematic Review With Pairwise and Network Meta-analysis of Closed Reduction Methods for Anterior Shoulder Dislocation. Ann Emerg Med. 2023 Apr;81(4):453-465. [pubmed]
- “MAP: Intra-Articular Posterior Shoulder Injection Tool.” Www.acep.org, www.acep.org/patient-care/map/map-intra-articular-posterior-shoulder-injection-tool/. Accessed 7 Jan. 2024.
- Smith, Clay. “And the Best Shoulder Reduction Award Goes To…” JournalFeed, 26 May 2023, journalfeed.org/article-a-day/2023/and-the-best-shoulder-reduction-award-goes-to/. Accessed 7 Jan. 2024.


