Slowww Down, Man. Myxedema Coma: A Case and Review
April 1, 2024
Myxedema Coma is a rare but life threatening endocrine emergency that we must be prepared to diagnose and treat in the emergency department. Buckle up for an in-depth discussion of a complicated emergency department case in an oral boards format with a focus on clinical reasoning, differential diagnoses, and ultimately a review of Myxedema Coma.
Contributors: Dillon Warr, MD and Jason Hine, MD.
Slowww Down, Man. Myxedema Coma: A Case and Review – The SimKit Podcast
Practicing procedures can be tough. Let SimKit do all the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. Get 10% off with coupon code SimKit10

The Case
History
A 69-year-old male presented to the emergency department overnight by EMS with a chief complaint of altered mental status. Per chart review, the patient had a history of ESRD on hemodialysis, hypertension, alcohol use disorder (documented at 1 pint per day), and hypothyroidism.
Per EMS, the patient was last seen normal by his sister 4 days before his presentation. He was found the day of his presentation by his landlord confused and disoriented. EMS reported the patient likely missed several dialysis sessions. Also known to still drink heavily.
History from the patient was quite limited by the patient’s disorientation and incoherent speech. However, he personally denied pain.
Patient was noted to have a similar presentation 7 months prior, where he also was found minimally responsive at home, found to be confused, with hypoglycemia, and volume overloaded from missed dialysis. His symptoms improved after multiple dialysis sessions.
Vitals
Initial set of vitals: HR 20s-30s, SBP 80s, RR 16, SaO2 98% on 6L NC. Noted to have undetectable temperature on the bedside thermometer and was frigid to touch (The outside ambient temperature was around ~25 degree Fahrenheit [-4C] the day of presentation).
Accu Chek: 14 mg/dL
Physical Exam
- HEENT: Atraumatic, PERRL, Unable to properly assess EOM given patient not following commands. Enlarged and swollen tongue + lower lip. Tolerating secretions. Uvula midline. No erythema.
- Cardiovascular: Bradycardia, tunneled hemodialysis line located right anterior chest.
- Pulmonary: No respiratory distress, Coarse crackles bilaterally
- Abdominal: Soft, nontender, non-distended
- Musculoskeletal: 2+ pitting edema bilateral lower extremities. Mild anasarca
- Skin: Skin is dry, cool to touch, without erythema
- Neurological: AO x 2 (self, hospital). Incomprehensible speech, moving all extremities equally. Could not assess gait or FTN.
ED Interventions in this Case
- Given an amp of D50 with repeat glucose normal.
- EKG obtained with sinus bradycardia and prolonged QTc.
- Given concern for hyperkalemia in the setting of missed dialysis, 2g IV calcium, sodium bicarb, Lokelma was given empirically. Insulin/Dextrose deferred due to hypoglycemia. Bradycardia did not improve until it transiently improved with 1 dose of atropine.
- Placed on Bair Hugger (active warming blanket for undetectable temperature).
- Bedside ECHO with good EF, no pericardial effusion, diffuse B-lines
- Stat CT Head ordered
- Nephrology consulted for emergent ED dialysis and the patient was placed in a HD capable ED room.
Quick Med Reconciliation: Amlodipine, Aspirin, Famotidine, Levothyroxine (last filled 3 months prior).
While awaiting dialysis, laboratory work-up and further imaging resulted:
CXR notable for b/l infiltrates c/w pulmonary edema
CTH without acute process
Na 141, K 6.0, Cl 114, HCO3 14, BUN 95, Cr 13.7
WBC 8.9, Hb 7.9 (stable), PLT 273
BNP 1791 (very elevated)
Troponin 14 (~ mild elevation, stable from prior)
Mild elevation in transaminases
Lactate 0.8
VBG 7.16/41/50/15
TSH 9.8 (elevated), T4 eventually resulted as very low
Blood cultures pending
Admitted to the ICU for further management, with hemodialysis in process
Summary:
A 69 y.o patient with history of ESRD, alcohol use disorder, hypertension, and hypothyroidism presented in mid-winter with altered mental status and hypothermia with associated hypotension, bradycardia, and hypoglycemia as well as evidence of volume overload, pulmonary edema, uremia, and hyperkalemia who was ultimately admitted to the ICU while undergoing hemodialysis.
Differential Diagnoses Considered
- ESRD with missed dialysis leading to volume overload with hyperkalemia and uremic acidosis
- Sepsis
- Alcohol use disorder with alcoholic ketoacidosis or starvation ketosis +/- Wernicke’s Encephalopathy
- BRASH syndrome (bradycardia, renal failure, AV nodal blockade, shock, and hyperkalemia)
- Calcium channel blocker overdose
- Environmental Exposure
- Myxedema Coma: A potentially unifying diagnosis. Hypothermia, hypoglycemia, bradycardia, and hypotension, especially in the setting of known hypothyroidism, as well as tongue swelling/lip swelling, could be a manifestation of myxedema coma
- Multifactorial
Next Steps
Given clinical suspicion by the ED and ICU team, endocrinology was called in the middle of the night for this possible endocrine emergency. They agreed that although the presentation was likely multifactorial, myxedema coma is a likely unifying and high risk diagnosis that required immediate treatment.
Endocrine Recommendations:
- Check Cortisol, ACTH, Free T3 BEFORE initiating treatment
- Give hydrocortisone 100mg q8hr, ASAP after laboratory studies drawn
- Follow with Levothyroxine 300mcg IV now, with 100 mcg daily afterwards
- Defer IV T3 given other possible etiologies, patient’s age, and his comorbidities
Case Conclusion
By the time the laboratory studies were drawn and the medications arrived from the pharmacy for administration, the patient had finished his emergent dialysis session. He remained altered and bradycardic with a HR in the 40s. In addition, despite several hours on the Bair Hugger, the patient’s temperature was finally read and registered at 93F. This lent additional credence to the diagnosis of Myxedema Coma.
Patient was subsequently admitted to the ICU for further management and close monitoring while receiving thyroid replacement, steroid therapy, and supportive care, including additional hemodialysis.
Myxedema Coma: A Review
Epidemiology
- Rare, fatal condition resulting from long-standing hypothyroidism of any cause; ie: congenital, iodine deficiency, autoimmune disease, or medications (lithium, amiodarone, etc).
- Mortality rate is reported from 20-25% to as high as 60% in some studies, even with intensive care. This is an endocrine emergency.
- Very rare: 0.22/1,000,000 per year in the Western World. More common in females and individuals over 60 y.o. More common in the winter.
Etiology
- Disrupted homeostasis in hypothyroid patients. There is usually a precipitant, including things like infection, trauma, drugs (amiodarone, lithium, beta-blockers), CHF, CO2 retention, hypoglycemia, and hypothermia.
- Some of the presenting symptoms could be a result of or a trigger for myxedema coma.
Pathophysiology/Presentation
Thyroid hormone influences virtually every cell in the body through gene modulation as well as directly affects cellular metabolism. Thus, an absence of thyroid hormone impacts multiple organ systems
Most commonly, it’s a female patient presenting in the winter with a history of thyroid disorders and a precipitating illness.
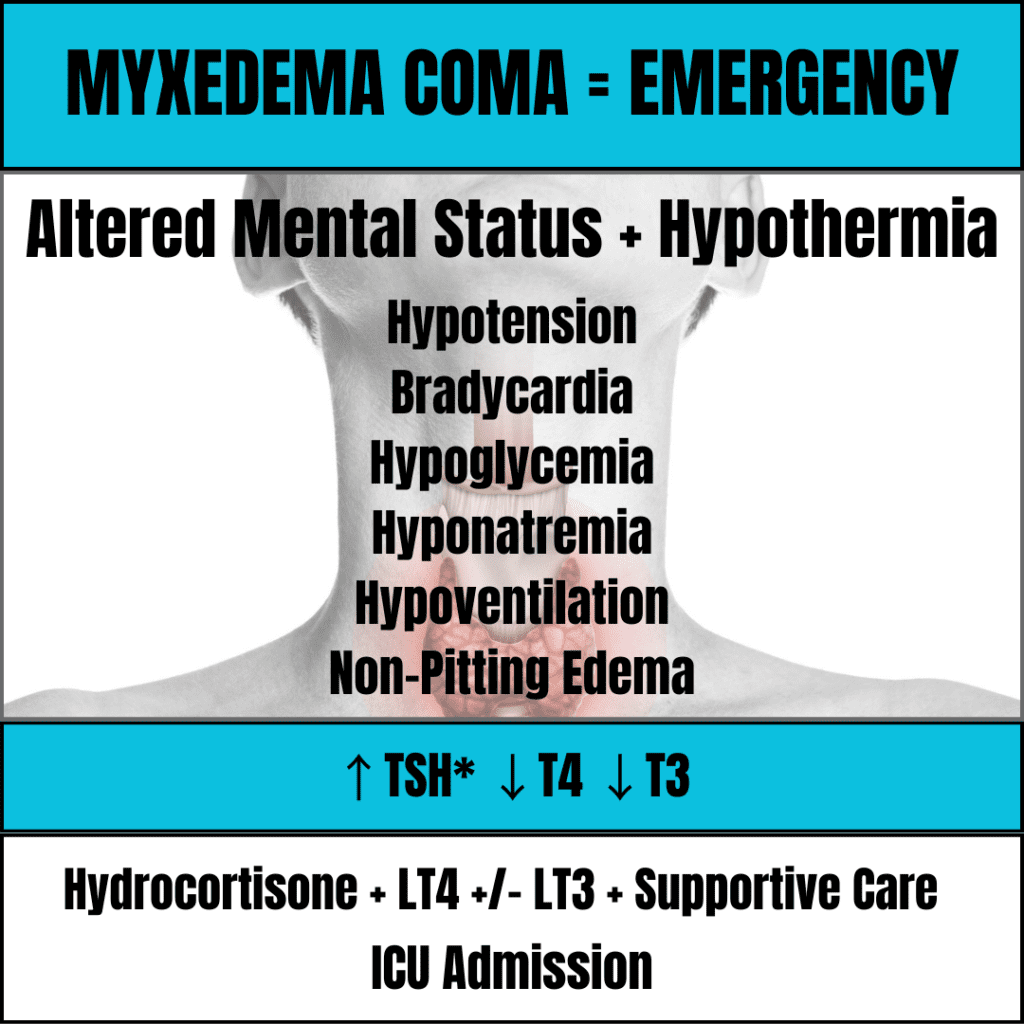
Two most common findings: Altered Mental Status and Hypothermia
Key Physical Exam Signs: Altered mentation of any kind. Dry, cool, skin. Non-pitting edema/puffiness, Bradycardia. Delayed DTRs.
Key Additional Features: Hypotension, bradycardia, hypoglycemia, hyponatremia, and hypoventilation
Neurologic
- Spectrum of effects leading to depression, disorientation, decreased DTRs, psychosis, agitation, slow mentation. Rarely seizures. “Coma” is a misnomer as it is not a very common neurologic manifestation.
- Multifactorial: Direct neurologic effects, hyponatremia, and hypercapnia
Hypothermia
- It is due to the loss of thyroid hormone-mediated thermogenesis that accompanies the decrease in metabolism.
- The severity of hypothermia is related to mortality in severe hypothyroidism; the lower the temperature, the more likely a patient is to die.
Bradycardia/Hypotension (Cardiac)
- Loss of thyroid hormone leads to decreased myocardial contractility, reduced cardiac output, and conduction abnormalities
- Can develop a pericardial effusion
Hypoglycemia (GI/Endocrine)
- Loss of thyroid hormone leads to decreased myocardial contractility, reduced cardiac output, and conduction abnormalities
Hypoventilation (Respiratory)
- Central depression of respiratory drive as well as from diaphragmatic weakness, leading to hypoxic and hypercapnic respiratory failure.
- Tongue swelling/lip swelling can contribute to respiratory failure from OSA
- Also can have pulmonary edema/effusion from decreased cardiac output
Hyponatremia (Renal)
- Hyponatremia a key finding
- Approximately one-half of patients with myxedema coma have hyponatremia. It can be severe and may contribute to the decrease in mental status.
- Patients have an impairment in free water excretion due to inappropriate excess vasopressin secretion or impaired renal function
Diagnosis
- Most commonly, laboratory evidence of severe, primary hypothyroidism.
- Severely low total T4, free T4, and free T3 and elevated TSH.
- Be cautious about excluding myxedema coma with a normal TSH if it’s high on your differential as an inappropriately normal TSH could reflect central hypothyroidism.
- In addition, the degree of TSH elevation may not be an accurate indicator of the severity of the hypothyroidism, as there are a wide range of TSH values seen in the literature.
- Other laboratory abnormalities: elevated transaminases, hyperlipidemia, hypoglycemia, hyponatremia, elevated CK, and anemia/leukopenia.
- EKG can show bradycardia with non-specific changes, variable blocks, or prolonged QTc
- There is a scoring system from a retrospective study derived from 21 patients, that includes alterations of thermoregulatory, CNS, cardiovascular, GI, and metabolic systems and the presence/absence of a precipitating event. May be useful in thinking about the disease but is limited in its application given its lack of external validation and small sample size.
Treatment
Guideline recommendations are based on case reports and expert opinion given the rarity of myxedema coma and the resulting lack of RCTs
Key Interventions
- Draw baseline cortisol, ACTH, T4, and FT3
- Hydrocortisone: “Stress dose steroids”. Often initiated at 100 mg IV loading dose, with doses ranging from 200mg to 400mg daily. Give before thyroid hormone, as thyroid hormone could precipitate an adrenal crisis as levothyroxine will increase cortisol metabolism. Hypothyroidism may also mask an underlying adrenal insufficiency.
- IV Levothyroxine (LT4). Initial dose is a one time IV dose of 200 to 400mcg (lower dose if elderly, underlying cardiac disease, or other comorbidities), with subsequent dosing at 1.6 mcg/kg/day (reduced to 75% IV) given daily thereafter
- IV Liothyronine (LT3). Given the possibility that T4 conversion to T3 may be decreased in patients with myxedema coma, can consider adding this to the hydrocortisone and levothyroxine therapy. However, recommendations in the most recent guidelines are weak, and caution must be exercised in patients with underlying heart disease given a risk of arrhythmia and MI and some studies reporting increased adverse outcomes. Can consider adding if at 24-48 hours there is no improvement in mental status or thyroid hormone levels still remain low, or TSH does not trend down.
- Therapy can and should be instituted based on clinical suspicion alone and should not be delayed while waiting for blood test results
- Can follow T4, FT3, and TSH every 24 to 48 hours until the patient’s mental status improves.
- Therapeutic endpoints in myxedema coma should be improved mental status, improved cardiac function, and improved pulmonary function.
Other Important Interventions
- Endocrinology consultation is necessary on clinical suspicion given the severity and potentially high mortality of this disease process. They can help to confirm your suspicions and provide assistance with medical management.
- Identify and treat the precipitating factor.
- Supportive care, including IVF for hypotension, antibiotics if infection is suspected, and mechanical ventilation of the patient is unable to protect their airway or has worsening hypercapnia/hypoxemia.
- Treat hypothermia with active rewarming such as warming blankets (Bair Hugger).
- Rewarming can cause vasodilation and worsen hypotension, so rewarm cautiously.
- Treat hypoglycemia and hyponatremia carefully, balancing the need for fluids for hemodynamic stability and need to treat hyponatremia without overcorrection.
Disposition
Given the high mortality rate, all patients should be admitted to the ICU. Even with intensive care, patients can die from GI bleeding, sepsis, or respiratory failure.
References
- Elshimy G, Chippa V, Correa R. Myxedema. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545193/
- Roberts CG, Ladenson PW. Hypothyroidism. Lancet. 2004;363(9411):793-803. [pubmed]
- Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, Cooper DS, Kim BW, Peeters RP, Rosenthal MS, Sawka AM; American Thyroid Association Task Force on Thyroid Hormone Replacement. Guidelines for the treatment of hypothyroidism: prepared by the american thyroid association task force on thyroid hormone replacement. Thyroid. 2014 Dec;24(12):1670-751.[pubmed]
- Popoveniuc G, Chandra T, Sud A, et al. A diagnostic scoring system for myxedema coma. Endocr Pract. 2014;20(8):808-817. [pubmed]


