Fat to Fab- Ozempic, Trulicity, the Celebrity Weight Loss Craze with GLP-1 agonists and what it means to Emergency clinicians
May 20, 2024
Ozempic and its counterparts, the GFP-1 agonists have been part of a huge celebrity weight loss craze. This has led to many to see these medications as a get-skinny-quick option and are pursuing these medications like crazed fans- leading to drug shortages. While these meds have an actual FDA indication of diabetes or obesity, individuals without indications for them, or those with indications but no prescriber, are turning to medical spas, weight loss clinics, and even compounding pharmacies to get their hands on Ozempic and other GLP-1 agonists. But these meds carry a side effect profile, and given their popularity it is likely some of those taking these medications may wind up in your Department.
In this vodcast we review these medications, their mechanism of action, and common side effects that might land a patient in the Emergency Department.
Transcript
This material for reference and visual purposes only, since it is authors associated seniority for minimization, planning, knowledge, materials or techniques shown or described unit. Its authors assume responsibility for patient safety outcomes, comma experience as guidelines to determine the procedure and processes in each individual patient.
Hello everybody I am Jason Hine. I’m an emergency medicine physician and the founder of SimKit. Welcome to this podcast and vodcast Fat to Fab, Ozempic, Trulicity, the celebrity weight loss craze and what it means for Emergency clinicians. So first we should talk about what this is not going to be about. This is not going to be a lecture or talk about fat shaming. 40% of patients presenting to the emergency department, 40% of Americans suffer from obesity, 11% from diabetes. The medications we’re going to be talking about today can have a real impact on the quality of life, morbidity and even possibly mortality for these patients when they’re prescribed in the right setting for the right reasons. Unfortunately, they are often being prescribed in the wrong setting and for the wrong reasons. We’re going to talk about that in a bit.
But with all that in mind, I want to introduce you to Amanda. Amanda is based on a patient I actually saw. She’s 43 years old. And she’s had some stubborn belly fat that she’s been trying to get rid of for a while. She’s gone to her primary care doctor a few times and she continues to get diet and exercise diet and exercise portion restriction. She’s tried that the best she can and simply cannot get rid of the weight. So with that in mind, she turned to a friend who she note has had significant success in the weight loss realm and asked what her secret was. And her friend said the secret is Ozempic.
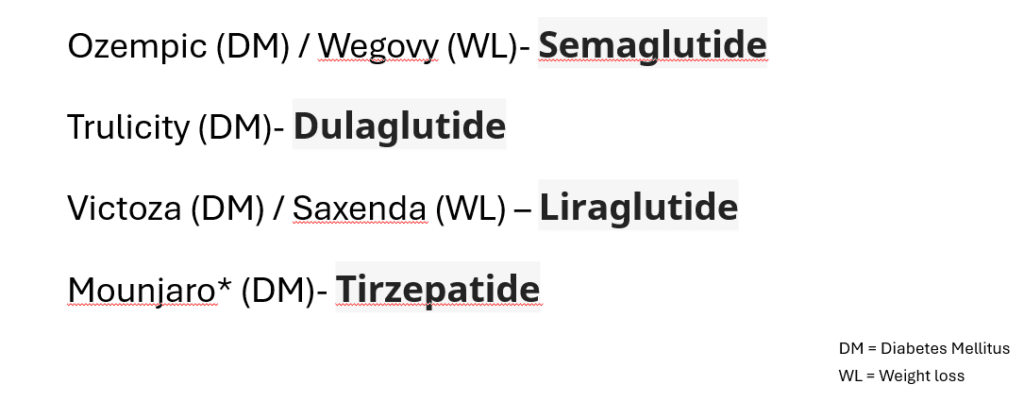
So what medications are you talking about today? We are going to be talking about the GLP1 agonists. We have semaglutide, dulaglutide, liraglutide, tirzepatide or Mounjaro, which is actually a GLP 1 and a GIP. But all these medications do fit into the category of a GLP1 agonists. They are all subcutaneous injections and they can be prescribed for either diabetes or weight loss. There is an oral form of semaglutide out there as well.
So how do these bad boys work? What is their mechanism of action? In our bodies, they are incretin hormones that are released in the small intestines after a meal. They work by potentiating insulin release to decrease any hyperglycemia we might have after eating. They also reduce gastric emptying and probably most importantly for weight loss, they decrease our intake or our calorie consumption by increasing our sensation of satiety by mechanisms in the central nervous system. And very importantly, listen up to this, patients prescribed a GLP 1 agonist on average will lose 15 per cent of their body mass, 15 per cent. If that catches your attention, it has definitely caught attention of others, particularly in Hollywood.
There has been a huge, huge celebrity craze related specifically to Ozempic, but to many of the GLP 1 agonists. There’s been a lot of speculation about who is and who is not using the medicine to try to get skinny, get fit for the runway or for beach season. Now I don’t know if Kim Kardashian or any of her family members are taking these agents, but there are several celebrities who have come out and spoken about their success using a GLP 1 agonist. One such person is the great Tracy Morgan from 30 Rock. Sharon Osborne has also spoken out about her success in weight loss with GlP 1 agonists and Charles Barkley as well.
So with the celebrity craze and the news related to these medications, the general populace has gone wild trying to get access to these medicines. Sometimes unfortunately, as a get skinny quick get ready for beach season or for that bikini bod right in time for summer. With that there have been significant shortages and access issues related to these medicines. Publications in the Wall Street Journal, even in vogue about how people are having a difficult time accessing these medicines, which is obviously very unfortunate for patients being prescribed them for the right reasons. Significant obesity. Diabetes in particular, not having access to the medicines that they truly need.
So how do you get prescribed this medicine? Are these medicines from the FDA standpoint? The first indication for weight loss anyways would be a BMI greater than 30. Or a BMI greater than 27 with an associated medical condition, including hyperlipidemia hypertension, for example. Who are these medicines not for? They are not for pregnant patients. Patients at risk for multiple endocrine neoplasm or medullary thyroid cancer. Patients at risk or have a history of pancreatitis, we’ll come back to that again. Patients with gastroparesis, because of the gastric emptying effect. And patients with inflammatory bowel disease. Patients with these histories should not be prescribed GLP 1 agonists.
So we talked about how this is in the lay press a lot, but this is also in our own press in the medical literature. The American Gastroenterological Association’s 2022 practice guidelines state specifically, patients who have inadequate response to lifestyle interventions. They recommend Ozempic as a first line therapy, so we definitely need to be familiar with this, not just because of patients looking for it, but because of our own societal recommendations.
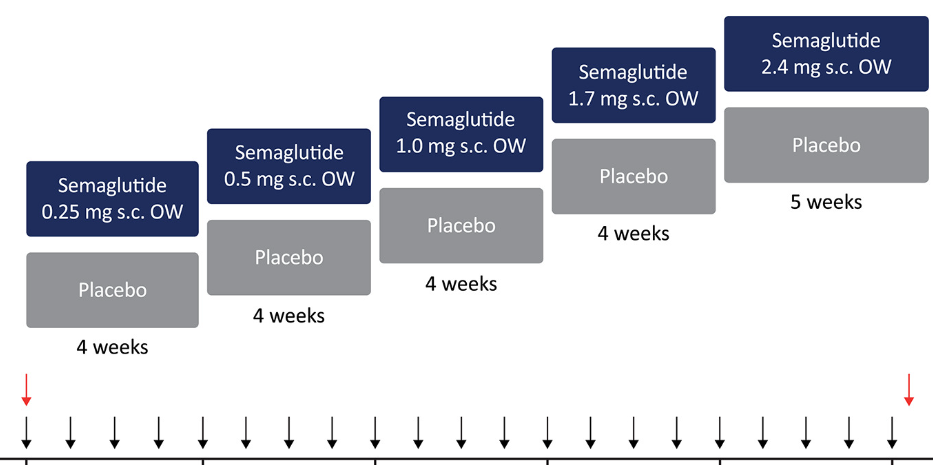
And in terms of dosing, the dosing structure is a four week gradual increase with the basic doubling of the dose every four weeks. It’s again once a, I’m sorry once a week injection subcutaneously starting at .25 milligrams and working your way up to a 2.5 milligram dose once weekly. This is worth noting because at times of transition or dose escalation is a common time to see more serious side effects.
So let’s come back to Amanda, our patient. So after talking with her friend who got on Ozempic and had success, she asked how she was able to get prescribed this medication. And amazingly to me she was sent to a concierge weight loss doctor. I didn’t know we had those in our area, but apparently we do and she was started on Ozempic. She has a little bit of issues in the beginning. But comes in shortly after a dose increase like we just mentioned, with significant side effects, particularly in the GI area- nausea, vomiting and diarrhea, and she felt quite dehydrated. So patients are definitely going to be coming in with side effects from these medicines and we need to be prepared to care fort hem.
So what are these side effects going to be? By far the most common are going to be GI 70 percent, 70% of patients on a GLP 1 agonist will experience GI side effects. Most commonly, these are going to be nausea, vomiting, diarrhea, or interestingly, constipation and abdominal pain. Now the odds ratios for these are not too, too bad. Three to seven or so for these numbers, but note that lots of patients, the majority are going to have some degree of GI upset. What other side effects can we expect? Metabolic ones can be present. If these medicines are mixed or used in conjunction with a Symphonia area or insulin, hypoglycemia can occur.
Other side effects are going to include hypersensitivity reactions now, by far the most common here are going to be local site reactions, including warmth, peritus, erythema, irritation, now, angioedema and anaphylaxis have been reported, but these are more noted in the extending. Analog versions kind of the older version of these medicines and are less reported in the human analog versions. The medicines we’ve been talking about today. And then we have to pay attention to access and compounding with people turning to medical spas, concierge doctors, weight loss clinics and even compounding pharmacies to get these medicines prescribed and to themselves, there’s going to be issues in terms of medication reconciliation, contraindications. And with these compounding pharmacies, pharmacies even dosing errors can occur. So we definitely need to be cognizant of that.
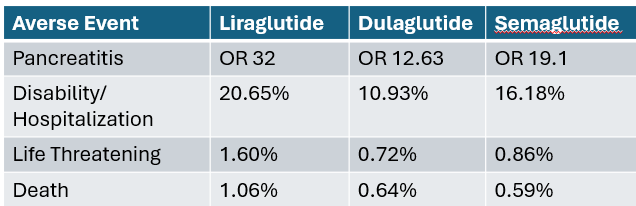
Now, what are the more serious side effects we might see in the emergency department because of the GI losses, dehydration and hypotension can be a common manifestation for sure. With that, and AKI is something to be conscious of now. Most of these are going to be pre renal again because of the dehydration. But it is worth noting that acute tubular necrosis and interstitial nephritis have been reported with the GLP 1 agonists, so we need to be conscious of intrinsic renal disease as well. And this is going to be more common in patients who are at risk for renal dysfunction. Pancreatitis is a well known side effect of these medications. The odds ratios for this are pretty profound. 12 to 32 odds ratios, with liraglutide having the highest incidence of pancreatitis. Something we need to be conscious of when patients come in with GI side effects, particularly obviously abdominal pain related to use of these medicines. Small bowel obstructions, possibly related to the gastric motility changes. And biliary pathology, it’s kind of an interesting one. There’s been some data suggesting that it is more common and than some observational studies recently that showed that it’s maybe not above baseline if it is going to occur, it is more likely in patients that have been on the medication longer for 26 weeks or longer or who are of course on higher doses. And who have lost significant amount of weight rapidly. Now, very importantly for me in understanding these medicines is how common are these complications and how serious can they be? There is an FDA adverse event report paper that’s out there which will be referenced in the show notes now. They talked about disability and hospitalization. Unfortunately, they did not define. Disability very well, but the numbers were quite remarkable for liraglutide, there is a 20% disability or hospitalization rate for semaglutide 16. Now do I think 20% of patients on liraglutide are getting hospitalized? No, I think that’s an overestimation and probably related to that strange or loose term for disability. But it is worth noting that these side effects can be quite severe. Luckily, life threatening side effects or death were very uncommon.
So in summary, these are common and popular drugs which have led to shortages, particularly for patients who really need them. The most common side effects are going to be gastrointestinal. Remember, 70% of patients will have some degree of GI side effects. That will include nausea, vomiting, diarrhea or Constipation and abdominal pain. Hypersensitivity reactions, particularly local injection site reactions, are going to be common. Anaphylaxis. Angioedema are going to be less cell. The more serious side effects that we need to consider in the emergency department include pancreatitis pre renal or intrinsic AKI, small bowel obstruction, possibly biliary pathology and hypoglycemia, particularly when mixed with other medications. And we really, really need to be paying attention to the prescriber and the access when a patient comes in on a GLP, one agonist, if we’re looking at medical spas or concierge doctors, we have to think about are they doing their due diligence and medication reconciliation, contraindication assessment and if they’re using in a compounding pharmacy. Are the doses accurate? And it isn’t actually the right medication. Collectively, these medicines can have a profound impact on the weight of patients suffering from obesity. They have the potential to affect their quality of life, their morbidity. But we need to be conscious of how they’re being used. The craze surrounding them, and people getting them for off label indications. I hope this helps inform your care of patients on GLP 1 agonists and I look forward to talking to you soon.
Keeping your skills up in rare procedures is an uphill battle. The Sim Center or conference small group once a year (… or 2 years… or 5!) is not enough. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off.
The GLP 1 Agonists Have Hit The Lay Press
Semaglutide (Ozempic) and its siblings the GLP 1 agonists have made it into the popular press in a big way. With many celebrities showing off significant weight loss and better bodies, thousands of Americans and people across the world are scrambling to get their hands on these meds to loss some unwanted weight. But these medications are not without their consequences.
The Big Players
While Ozempic seems to be getting most of the press these days, there are several agents on the market for weight loss and diabetes
Dosing
The dose adjustment for sumaglutide is as shown below. Dose increases occur every 4 weeks until the patient reaches 2.4 mg subQ once weekly or is stabilized at a lower dose.
Side Effects
These medications are not without their side effects. The ones to be familiar with are:
- Gastrointestinal– an impressive 70% of patients will report GI side effects. These can include nausea, vomiting, abdominal pain, diarrhea or constipation.
- Hypersensitivity– the most common of these are going to be local site reactions like warmth, pruritus, and erythema. While angioedema and anaphylaxis have been reported with GLP 1 agonists, this was more common with the older exendin-analogs, less common with the newer human-analog drugs.
- Metabolic– when these medications are mixed with a sulfonylurea or insulin, hypoglycemia can occur.
- Access and Compounding– with people turning to weight loss clinics, medical spas, and concierge doctors for their prescriptions, drug-drug interactions or contraindications may be missed. With compounding pharmacies potentially being used do to shortages, dosing errors need to be considered.
- Serious– the more serious side effects of these medications to consider and screen for are:
- Dehydration/hypotension– with the GI losses patients may experience dehydration and possibly even resultant hypotension
- Acute kidney injury– many of these will be pre-renal in nature from the losses, but acute interstitial nephritis and acute tubular necrosis have been reported with liraglutide.
- Pancreatitis– this is a well established complication of these medications with Odds Ratios in the 16 to 32 range!
- Small bowel obstruction– this adverse effect has been reported, possibly due to the change in gastric motility.
- Biliary pathology- biliary colic and cholecystitis have been seen, with variable reports from increased rates to not above the general population. If it is going to occur, it is more likely in patients on a higher dose, who have been taking it longer (>26 weeks), and who have had significant weight loss.
How common, exactly?
The table below is from a FDA Adverse Event Reporting paper [2]. Now unfortunately they did not define disability well, and I believe the numbers for Disability/Hospitalization are therefore elevated, but still impressive numbers to consider when seeing a patient with side effects from a GLP 1 agonist.
Summary
GLP 1 agonists are common and popular drugs, which has lead to shortages and issues with access. The most common side effects are GI (including nausea, vomiting, diarrhea/constipation, and abdominal pain), but consider hypersensitivity reactions (including uncommonly angioedema and anaphylaxis), hypoglycemia when GLP 1 agonists are mixed with sulfonylurea or insulin, and issues related to access such as medical spas where medication reconciliation and contraindications may not be as thorough. More serious side effects can include significant dehydration, acute kidney injury, pancreatitis, small bowel obstruction, and biliary pathology. Finally, consider the issue of compounding pharmacies and dosing errors when seeing a patient with side effects from a GLP 1 agonist.
References
- Long B, Pelletier J, Koyfman A, Bridwell RE. GLP-1 agonists: A review for emergency clinicians. Am J Emerg Med. 2024 Apr;78:89-94. [pubmed]
- Liu L, Chen J, Wang L, Chen C, Chen L. Association between different GLP-1 receptor agonists and gastrointestinal adverse reactions: A real-world disproportionality study based on FDA adverse event reporting system database. Front Endocrinol (Lausanne). 2022 Dec 7;13:1043789. [pubmed]
- Friedrichsen M, Breitschaft A, Tadayon S, Wizert A, Skovgaard D. The effect of semaglutide 2.4 mg once weekly on energy intake, appetite, control of eating, and gastric emptying in adults with obesity. Diabetes Obes Metab. 2021 Mar;23(3):754-762. [pubmed]
- Rubino DM, Greenway FL, Khalid U, O’Neil PM, Rosenstock J, Sørrig R, Wadden TA, Wizert A, Garvey WT; STEP 8 Investigators. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022 Jan 11;327(2):138-150 [pubmed]
- Rubino D, Abrahamsson N, Davies M, Hesse D, Greenway FL, Jensen C, Lingvay I, Mosenzon O, Rosenstock J, Rubio MA, Rudofsky G, Tadayon S, Wadden TA, Dicker D; STEP 4 Investigators. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021 Apr 13;325(14):1414-1425 [pubmed]
- https://www.kbtx.com/2024/03/14/national-shortage-ozempic-leaves-many-without-essential-medication/
- https://www.today.com/health/celebrities-on-ozempic-rcna129740 accessed 3/16/24


