Keep ‘Em Cool, But Not Too Cool- AHA recs on TTM in post-ROSC care with Dr. Mike Burla
April 29, 2024
In this podcast we review the most recent AHA recs on TTM. The current AHA recently updated their practice guidelines related to targeted temperature management (TTM) in the post-ROSC patient…. and there really are some of nuances of caring for these patients. To review this, we spoke with Dr. Mike Burla, an EM physician with research experience in out-of-hospital cardiac arrest, and someone we have had as a guest for prior discussions on the topic.
Check out our first conversation with Dr. Burla here:
Post-ROSC Care with Dr. Mike Burla
Fat to Fab- Ozempic, Trulicity, the celebrity weight loss craze and what it means for Emergency clinicians – The SimKit Podcast
Transcript
Jason Hine: Hello everybody and Welcome back to the Sim kit podcast. I am excited to have a return guest. We’ve been having a couple of those lately. it’s cool. It’s exciting. I have a return guest today with me in Dr. Mike burla Mike and I chatted a while back, I guess in August about blood pressure considerations in the post arrest patient and where we might want their map to live. We also talked a bit in about temperature. talked about ttm2 and
Jason Hine: let’s see and we talked in that podcast a little bit in August 2023 about ttm2 and We are back to discuss societal recommendations, which seem to be changing with regard to temperature Management in the post- Ross return of spontaneous circulation patient. So Mike thanks for coming back to chat with me with us today. Tell us a little bit about what you’ve been up to you since we last talked and your role in these out of Cardiac Arrest patients and your research
Michael Burla: Thanks again for having me. It’s always a pleasure. I can’t remember exactly what we went over last time in regards to what’s happening at Maine health and specifically what’s happening with research of at a hospital Cardiac Arrest patients, but to give a quick summary Dr. Theresa May one of the intensivists at Maine Medical Center developed a program called the post Cardiac Arrest Learning Community or P Cal. and the purpose of the project was to come up with strategies to improve overall care of these post-ROSC patients specifically in the rule communities and the rule setting as it can be a little bit more challenging to care for these patients in that setting as there are several critical access hospitals in
Michael Burla: Throughout Maine that receive these patients and need to transfer them to definitive care. So we meet monthly to discuss case review and different ways. We can improve on the transition of care from emergency departments to the ICU emergency department, to transfer the ICU things of that nature.
Jason Hine: that’s fantastic. I mean These are high intensity High resource patients we work a lot in a community hospital that’s quite close to that Ivory Tower caring for them in a rural environment with a two three, however, many hour transport time and the amount of staff and care that they need in that time frame. It’s gonna be a lot so working with these people and these Community providers to make sure that they’re following best practices that they’re well supported and they’re getting their patients to a final disposition covering all the bases of what needs to be done. Sounds like a fantastic project. So thank you for the work you do there.
Michael Burla: for sure. again Dr. May, is hosting these meetings and it’s been an amazing body of work and something that I’m passionate about for me specifically. I’m looking at the process of these transferring of the me specifically I’m looking for
Michael Burla: for myself specifically. I’ve been looking at our process of actually transferring these patients out and to keep it short. We’ve looked retrospectively over the last couple of years to see what has been going on during these transfers are there physician orders or Vital sign parameters in place is their variation between different agencies and long story short as you know, we’re not seeing, any orders or very little orders. long story short, we’re not seeing any specific vital saying parameters in place when these patients are transferred it similar to how you would see,
Michael Burla: Let me take it from the time. For me for myself specifically.
Jason Hine: Yeah, go for it. No worries.
Michael Burla: I’ve been looking at our process of transferring these patients out. We looked retrospectively to see if there is any inconsistencies between physician orders and Vital sign parameters or difference between agencies and long story short. We found very little physician orders being placed and essentially no Vital sign parameters during the transport of these patients. And so I think an ideal situation, we have some protocolization, to try and optimize the care and get it as close as
Michael Burla: Possible to an ICU level care prior to arriving to the ICU and I would say similar to our stemi transfers, right? Those are very protocol eyes. you get the Plavix the Heparin drips the nurses ready to go. everything’s set up, to optimize the care and I would say, we’re trying to move course that Direction with these post-ross patients that I’ve been working with our colleague and our local EMS director Dr. Meehan Coussee that so
Jason Hine: Yeah, that’s fantastic and having those recommendations and I’m always a guideline person as opposed to a policy person because every patient’s different but just giving directionality of what we should do. What are best practices in terms of blood pressure temperature glucose all the things that we need to consider and I’d argue that these patients are more unstable and more prone to bad outcome from the care provided. Once they get a pulse back then the semi patient that is only in your department for a short period of time before getting their PCI.
Michael Burla: I would agree completely.
Jason Hine: Perfect. So Dr. Burla we are here largely to talk about the A recommendations that actually came out around the time of our initial conversation in August, and these are titled temperature management for comatose adult survivors of cardiac arrest a from a science advisory from the American Heart Association. In this publication, they put a lot of credence to ttm2 study and state quote. For unresponsive post Cardiac Arrest patients with characteristics similar to those of individuals included in the ttm2 trial out of Hospital card Of cardiac or unknown cause excluding those with unwitnessed asystole controlling patient’s temperature to less than 37.5. Celsius is a reasonable and evidence-based approach. Mike what are your thoughts on these recommendations?
Michael Burla: I think it’s reasonable for sure. I think they’re well thought out recommendations, and as we mentioned before the patient population in the ttm2 study was a fairly healthy population, predominantly without significant comorbidities. I was a majority male younger age, around 63 to 64 with low levels of diabetes hypertension and patients that experience to witness to rest with the shock couple Rhythm and when you don’t include unwitnessed arrest or initial rhythm of asystole or what they deemed as quote limitations in care I think when you focus specifically on this patient population that is known to have better outcomes, looking at the temperature range that they evaluated I think the statement makes a lot of sense. I think that it’s recognition that ttm2 was a very well done study and that those temperature ranges do appear to be applicable for that patient population. So, if we had a patient with a witness arrest and even more specifically with a shockable rhythm such as Vfib or VTach maintaining a temperature between 32 and 37.5 degrees Celsius does seem reasonable. I would say that the brief update does know that there is still recommendation that if the patient is not making purposeful movements, I not pulling for the tube or not following commands things of that nature. It is still recommended that patients have quote a deliberate strategy for temperature control. So, I think what we can take away from that statement is while this This specific patient population might not need as aggressive as cooling as we initially thought you simply can’t just forget about the temperature. It’s still a Vital sign where there needs to be some parameters in place at least based on the literature we have today.
Jason Hine: yeah, that makes sense and thank you for bringing up some parts that were in our initial conversation and for folks listening. We will have a link in the show notes to our initial chat on the topic, but for ttm2 like you had some legitimate reservations, and of course that being said that did not affect these updated recommendations we’re discussing now. So thanks for sort of bringing that to light. I think whenever we have these societal Rex we need to know Where the recommendation is coming from and it is essentially holy based on ttm2. A lot of the prior work showed a pretty prominent or pretty definitive benefit to Cooling.
Jason Hine: And cooling to a relatively cold degree, right? We initially were kind of at 30 to 33 and then we’ve seen some studies. maybe it’s 36 and now we’re basically between 32 and 37 degrees and you brought up one element that I think is worth highlighting again in thinking about these recommendations and thinking about TTM2. So the first of which is the applicability ttm2 is definitely the largest and a very well done study on targeted temperature control in someone who is post Cardiac Arrest who has risk.
Jason Hine: But recognizably, this was a Scandinavian study. And as you mentioned that patient population their protoplasm might be a little bit healthier than the average American who comes in post Rock and so knowing that and knowing the application of the data to the patient in front of you is super important. So knowing that it’s more witness arrests more V5 VTEC and in Scandinavians who had fewer comorbidities that said it probably and doesn’t seem to be affecting the recommendations for General care in America and other developed countries the other point that you brought up in our initial chat. I was hoping you could sort of tell us your thoughts on that now, is about
Jason Hine: Basically our progression in care of the post arrest patient, we had the Haka trial we had the Bernard trial ttm1 ttm2 and the Pendulum is a swing in my friend, right we are going from keeping them very cold to maybe not so cold to now just basically preventing a fever.
Michael Burla: Yes.
Jason Hine: And you made the analogy of sort of rivers and early goal-directed therapy and showing how that had such a profound impact and over time all of the elements of early gold directive therapy. We’re kind of chipping them away and maybe recognizing that it’s just a focus on the patient and really being cognizant of their progression in the emergency department. Tell me you’re sort of standpoint on that and how that might apply to the post-rosk patient.
Michael Burla: I think that kind of the progression of what we’ve seen in the literature does reflect when we think about sepsis and how we approach steps as patience and the Pendulum swinging back and forth between needing specific things that early goal directed therapy had that to now not needing those things and…
Jason Hine: Yeah, I’m not checking wedge pressures anymore,…
Michael Burla: Exactly, right and…
Michael Burla: perhaps are exactly prepped our approach to those patients are different and I do think the same can be said with this patient population. When we look at other Vital sign parameters and post rocks care. There are varying degrees of literature. Just that suggests the optimization of care.
Michael Burla: For instance, as we touched on with our first talk, aggressive blood pressure management specifically within the first couple hours of achieving Ross. There’s been evidence of improved outcomes and the A recommendations have guidelines based on that, but when we look at, strict glucose targets the studies that are been out there haven’t necessarily improved outcomes when you have a specific Target to avoid hyperglycemia, for instance. So whether you’re targeting a range of 140 to 160 or 1480, it didn’t really make a difference. However, the benefit of preventing hypoglycemia has been shown and so as long as you’re closely monitoring the glucose, so it doesn’t dip to a hypoglycemic State you’re likely providing some benefit and again, I think as we
Michael Burla: More and more studies come out about targeted temperature management hypothermia. I think from a temperature perspective, they’re similar statements can be made and again specifically with this patient population of witness to rest predominantly v-fib and vtach or shockable rhythm. whether you target 33 or 36 or even 37.5 degrees Celsius, it probably doesn’t make a difference. But as long as you’re closely monitoring the temperature to prevent degrees of hyperthermia pyrexia, there should be some benefit.
Jason Hine: That makes sense to me and I do see that as being a potential downside almost of this leniency and Temperature Control in that the time you spend in the room observing the patient and seeing their hemodynamics their purposeful movements Etc that matters right and if you are not as attuned to it back, years ago when we were trying to bring them down in temperature and we’re going in and out of the room to see for reaching our Target of cooling that might be the benefit right our time in the room our hands on patient our communication with the nurse. And so now that we’re kind of in more of a Let It Ride don’t let them get a fever algorithm or approach or protocol. There might be less time spent or less attention to the patient in that regard.
Michael Burla: Yeah, I completely agree. I mean, I think I can both speak on this, in a community setting, when you have one of these patients it’s very easy for people to get lacks about the situate. We got the first blood pressure’s 140 over 80 or something like that. we’re gonna get sedation. We’re gonna get this we’re gonna get that and then if you’re not necessarily glued to the bedside to make sure X Y and Z happen which like you said when we were really worried about getting specific targets. You were a little bit closer to the bedside if you leave and maybe now the blood pressure dips and no one’s really paying attention or maybe the temperature rises and you don’t have a bladder probe getting continuous temperatures or things of that nature and then now the patient you check back and they’re a little hypotensive maybe their febrile, that’s lost time and deviation in Vital sign parameters. You just can’t get back.
Jason Hine: Yep. Yeah that makes a lot sense to me and it is totally fair. So I think it’s gonna be a very conscious effort for providers who are now not as stringent about temperature control to make sure that they’re maintaining that touch point because we all know what happens in the department whether you’re single coverage or multi you have a poster occupation. They need two confirmation they need Central line, they need pressure starts. They need sedation starts. You put all this upfront work in you come out of the room to the four or five, level threes twos and…
Michael Burla: right
Jason Hine: whatever and then you have to go continue to provide care for the rest of your apartment. And if you don’t have specific points that you’re targeting and touch points that you’re mandated basically to do in these patients. They may fall by the wayside awaiting transport.
Michael Burla: exactly
Jason Hine: No, I wanted to ask you a little bit more in something. I found interesting. So an interesting part of the current recommendations is to maintain a targeted temperature range of 32c to 37.5. and specifically highlighting that lower limit of 32 in what we see in our data and ttm2 they’re probably is not a major benefit in hypothermia. So I suppose that this is based on the data that there’s no difference in the outcome between really cool and just normal thermic. So if it’s not worse to be really cool then I suppose it’s okay. It’s similar. Can you kind of give me your Takeaway on that range that they created in the new recommendations?
Michael Burla: So I think that part of it is just the lack of data on the out of Hospital Cardiac Arrest patient in general, and specifically unwitnessed arrest with asystole or pea, I know they weren’t initially. Looted in the recommendation of the temperature control, but if you look we know they have a worse prognosis and it’s a less steady population. there may still be some benefit to having, a cooler temperature in certain patient populations, but it’s just there hasn’t been enough studies done to suggest that which the brief update it does state that
Michael Burla: there’s quote insufficient evidence to recommend a specific temperature for different subgroups of patients with cardiac arrest and I think that’s directly referring to those, a systole unwitnessed arrests and so, when we think about out of Hospital Cardiac Arrest as a whole and not necessarily excluding or only including witnessed the tax hackable Rhythm arrests. I think at that point you really do need to lean on your local institutions protocols or recommendations, we still have a cooling pathway through Maine health and depending on the patient and the potential need for more no protectivity. We still have goals between 33 and 36 degrees now that
Michael Burla: Change at some point. But if you speak to our intensivists, that’s still something that’s in play. there just hasn’t been enough research done to really look at this. mean there are still studies being conducted. that do look at this strategy ice cap is one for instance, the influence of cooling duration on us can see in Cardiac Arrest patients. Now, they’re looking mostly identifying an optical duration of cooling but they’re including both witnessed and honor witness to know witness to rest who have experience out of Hospital cardiac arrest and I think that the more literature that is out there that includes this patient population the better understanding we’d have of what an ideal temperature range is because for now, yeah, it’s 32 37.5 so
Jason Hine: Yeah, and that’s quite the range and thank you for sort of bringing that to light a little bit because it isn’t interesting area of lack of data and I don’t fault ttm2 authors for excluding unwitnessed or as systolic arrests. You don’t want to have a dilutional effect in patients that are being kept Alive by epinephrine or have a very poor prognosis you want to be able to actually derive data of…
Michael Burla: Yeah.
Jason Hine: what can be beneficial in the lives and brains that can be saved. So I see why they targeted witnessed or V shot VTEC the FIB arrest, but that doesn’t mean that your patients aren’t gonna come in with the latter right?
Michael Burla: exactly
Jason Hine: It’ll be great to have that Scandinavian gentlemen straight off the cruise ship who comes in and goes down in front of people. They shock them out of it. That’s great purpose perfect applicability of TTM too, but we’re still gonna get Mema from the nursing home who was found.
Jason Hine: With unknown downtime with a systole who got pumped full of EPI and is now alive and we have to figure out how to manage her properly as well. And that’s an interesting wrinkle. It’s great to hear that. There’s actually Nuance to the care being provided through main Health. If you can speak a little bit more when we’re finding that lower target range to maybe be beneficial or who are the ideal patients for this neuro protectivity of hypothermia. yeah,…
Michael Burla: so I
Jason Hine: go ahead. Sorry.
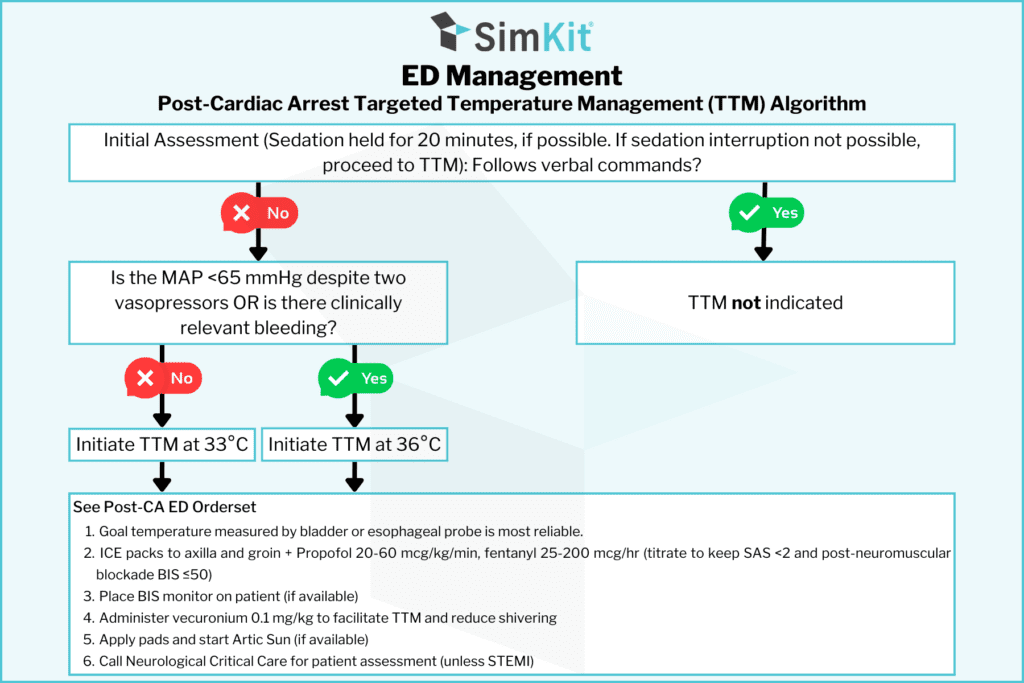
Michael Burla: it is more at the discretion of the intensivist, but generally speaking it’s patients who have the potential for more, risk of catastrophic neurologic outcomes. So, longer downtime, other factors that could relate to poor prognosis like comorbidities and a PA arrest as opposed to shockable Rhythm. So those sort of Things fall into place. We actually do have an algorithm that you would at least initially follow in the Ed or look at as a guideline. And then when you speak to the intensivist, they can give you a little bit better idea on which temperature to really Target generally speaking, somebody’s chemo dynamically unstable. That’s another thing to consider if someone’s on multiple pressers.
Michael Burla: and you’re still having a hard time achieving an adequate map. That’s another patient where different targets and temperature need to be in consideration where you wouldn’t necessarily want to cool them too much, just because it has the potential to change their human dynamics if they’re already still someone unstable. So that’s another Thing to consider that’s also in the algorithm. But at the end of the day, it does come down to vital signs or blood pressure aside comes down to where they think the patient is best served from a neural protectivity standpoint and at the end of the day, I mean we were just trying to do what’s best for the patients.
Jason Hine: That makes sense. And if I could pin you down maybe a little bit more on that mic. How are you currently handling the unwitnessed asystolic patient who comes into your poster ask?
Michael Burla: So, I would say being at least from a management standpoint initially aggressive as I can be from making sure their blood pressure making sure we can get a map above 80 making sure we’re oxygenating adequately and then from it an induction standpoint to cooling making sure that we’re getting them cooled as soon as possible now. Am I automatically targeting 33 degrees? I think that in the process of cooling, I’m on the phone with the intensivist pretty quickly to get some guidance but in the absence of guidance, yeah, at least I’ve certainly trying to prevent hyperthermia peroxia and our hyperthermia or
Michael Burla: undesirable temperatures, but at the same time if I’m
Michael Burla: I’m being aggressive treating the patient and trying to make sure that we decrease the time to their induction phase of cooling and in the absence of instructions. I’m still cooling to 33 degrees.
Jason Hine: Interesting, That’s helpful to hear and not to make light of the other things. I think that’s where three iterating all of the other parts of care and some of which we talked about in our prior podcasts are still very very important. So someone comes in poster ask you you guys Health have a relatively I’d say maybe aggressive. I don’t know. If you agree in terms of our map Target being somewhat High pushing toward 80 for a map making sure that they are not becoming hypo or hyperglycemic to make sure that they’re not at risk for hyperoxia or hypoxia. Those things come into play in all of these patients and then because ttm2 doesn’t really specifically cover. Temperature in these patients if you think that there is a benefit possibly to some neuroprotection related to mild hypothermia. It sounds like you’re driving those patients a little bit lower.
Michael Burla: Yeah, I think I wouldn’t delay transport or transfer to the ICU to achieve these goals. So if I got to 36 or even 35 and it was time to transfer the patient or get them up there, I would say that’s okay, but in the absence of knowing when the patients being transferred or, knowing when I’m able to get the patient out of the department, I am going to be again direction from the intensivist via phone. I’m gonna be as conservative in my opinion as I can be from a protect protection standpoint. and you’re right. I think main health does have some aggressive parameters, but
Michael Burla: the brief update and AJ does recognize that hospitals should come up with their own protocols for these patients. That might not all be the exact same, because when you look at the guidelines, there are varying degrees of values for different Vital sign parameters, which does include, map back in the 2020 guidelines.
Jason Hine: Yeah, that’s helpful to kind of go over as we get closer to a close just to summarize things and feel free to interject and correct as we go but looking at these ha recommendations basically coming off of ttm2.
Michael Burla: Okay.
Jason Hine: We’re seeing that the Temperature management pendulum as we mentioned it has swung relatively rapidly from quite cool to kind of cool to now a range of 32 to 37.5. We know from the data that we’re quite well supported in not driving them particularly low but most importantly avoiding pyrexia or fever in patients that have a generally healthy underlying.
Jason Hine: Medical history who have good protoplasm if they’re Scandinavian even better and…
Michael Burla: you better
Jason Hine: that have had a witness arrest and the Vifb VTach shockable Rhythm. They come back that is right down the pike of what ttm2 looked at and we are well supported in that range of 32 to 375 not seeing Significant benefit really in driving those temperatures lower but as we do that and as we think about other patients that will come across our department particularly the asystole patients or the unwitnessed arrest patients. The data is not as well founded. We don’t have as much support there and within that, relatively large range of 32 to 375 there might be play and there might be certain period
Jason Hine: there might be play and there might be certain patients that benefit from a lower level or a greater degree of neuroprotection. All of this should be done in consultation with our intensivists getting them on the horn early obviously to delay, the length of time in the department is very important Trying to minimize that and get to our targets get our patients stabilized for transport as early as possible. And in those conversations seeing what the intensivists who will be caring for the patient long-term thinks about their ideal range within that 32 to 375.
Jason Hine: Do you want to add anything that?
Michael Burla: I think that sums it up greatly. I think the main point towards the end, lean on your local institutions policies and protocols and what the ICU and the intensivists at your institution think from a Vital sign parameter standpoint. And again that’s well Illustrated in a brief update specifically because we don’t have great data on out of Hospital Cardiac Arrest patient as a whole when we include unwitnessed.
Michael Burla: Pea and asystole arrests and these patients are still coming to our doorstep and we’re still treating them. So, I think that’s a good, take home point that we can’t forget when it comes to this update.
Jason Hine: Perfect axon, so a collective summary about our conversation and our points of care in the post-rosc patient. We are focusing on temperature here that is the point of our podcast but we would be remiss not to mention the other elements that are very important. So making sure that you are keeping their oxygen in a stable range that they’re not hypoxic and we really don’t want them to be oxic either. We’re not driving 100% fio2 and a pulse oximetry of 100 either we want to be conscious of that conscious of glucose and map and working on with
Jason Hine: Tons of this on what the ideal Target map is going to be important as well when we come to temperature. That is our a recommendation that we are reviewing here. We see our temperature range of 32 to 375 and there might be nuances within that knowing the ideal patient for ttm2 again that witnessed arrest shockable Rhythm generally healthy that fits that there are other patients that we have to care for who are not going to fit that bill and we’re still going to exist within that 32 to 375 but a little bit more nuance and certainly something worth the conversation with your intensivists as you get ready for transfer and globally probably the most important take-home here is as we kind of made the analogy to early goal directed therapy.
Jason Hine: If we are becoming more lacks or less stringent in our temperature control, we cannot forget that that does not mean we set it and forget it and wait for the ambulance to arrive continue to care for the other patients. The touch points we have with our post-rosc patient are incredibly important for recognition of nuances that you might not see in a chart review or in a Vital sign Trend getting in the room laying hands on the patient working with your nurse to make sure you’re addressing all the things that they are seeing are coming up with our vitally important for the long term survival and the morbidity for these very sick patients.
Michael Burla: Exactly, and that’s what the AJ means by deliberate strategy having a strategy for these patients and sticking to it.
Jason Hine: Perfect. Dr. Burla, thank you again for coming on and chatting with us about these recommendations the work that you’re doing with our post-ross patients. I appreciate everything you do and taking the time to chat with us today.
Michael Burla: Thanks for having me.
Practicing procedures can be tough. Let SimKit do all the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. Get 10% off with coupon code SimKit10
The Pendulum is A-swingin’
The ideal temperature for the post Return of Spontaneous Circulation (ROSC) patient has been a moving target. Since the days of HACA and Bernard et al., we have been cooling post-ROSC patients with the belief in neuro protection. Then TTM1 came out and brought that into question. Finally, TTM2 was published in 2021 which largely refuted the benefits of cooling, but there are some significant caveats related to the patient and their presentation. From this, our current AHA recommendations are for a target temperature between 32-37.5 degrees Celsius.
Who TTM2 looked at, and Who they didn’t
In TTM2, the authors tried to avoid the dilutional affect of patients that come in with a profoundly poor prognosis which would hide a signal of benefit to cooling in those that can be saved.
To do that, they excluded patients with unwitnessed arrests and those PEA or asystole on presentation.
This left them looking at patients with witnessed arrests and Vfib or pulseless Vtach. This was also a Scandinavian study, and patients were (unfortunately) generally healthier than the average American who comes in post-ROSC.
Treat Them Differently?
This leads us to an interesting dichotomy in our patients.
On the one hand there are those who are generally younger, healthier, and have witnessed arrests and Vfib/Vtach when people put the pads on. In light of TTM2, we can say these patients likely don’t benefit from cooling to a lower target like 32-33 Celsius. In these cases, avoiding fever or hyperthermia is the goal and this is supported by the well conducted TTM2 trial.
But what about MeMa from the nursing home who is found arrested, has asystole or PEA on initial assessment, but comes back? Unfortunately, despite her poor prognosis, we still have to care for her despite dearth of evidence on how cool to make MeMa. In these circumstances, Dr. Burla recognizes there still may be a neuro protective effect of cooling and, in consultation with our ICU colleagues, may be someone we bring to a cooler temperature within that range of 32-37.5 degrees Celsius.
Get With The Guidelines
Clearly, the care of these patients is nuanced and we should not be acting in a vacuum or making individual decisions when the care of these patients will ultimately be transitioned to our ICU colleagues. With that in mind, it is highly recommended to consult our intensivists early and determine cooperatively the ideal temperature for the patient in front of you.
Ideally, guidelines in care are established before the patient hits your door. One such Guideline can be found below.
Check out more on the topic from friend’s of SimKit!
Emergency Medicine Cases: Episode 72 ACLS Guidelines 2015 Post Arrest Care
References
- Perman SM, Bartos JA, Del Rios M, Donnino MW, Hirsch KG, Jentzer JC, Kudenchuk PJ, Kurz MC, Maciel CB, Menon V, Panchal AR, Rittenberger JC, Berg KM; American Heart Association Emergency Cardiovascular Care Committee, Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Peripheral Vascular Disease; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, and Stroke Council. Temperature Management for Comatose Adult Survivors of Cardiac Arrest: A Science Advisory From the American Heart Association. Circulation. 2023 Sep 19;148(12):982-988. [pubmed] open access- AHA journals
- Perman SM, Elmer J, Maciel CB, Uzendu A, May T, Mumma BE, Bartos JA, Rodriguez AJ, Kurz MC, Panchal AR, Rittenberger JC; American Heart Association. 2023 American Heart Association Focused Update on Adult Advanced Cardiovascular Life Support: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2024 Jan 30;149(5):e254-e273. [pubmed] open access- AHA journals
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002 Feb 21;346(8):549-56. [pubmed]
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002 Feb 21;346(8):557-63. [pubmed]
- Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, Pellis T, Stammet P, Wanscher M, Wise MP, Åneman A, Al-Subaie N, Boesgaard S, Bro-Jeppesen J, Brunetti I, Bugge JF, Hingston CD, Juffermans NP, Koopmans M, Køber L, Langørgen J, Lilja G, Møller JE, Rundgren M, Rylander C, Smid O, Werer C, Winkel P, Friberg H; TTM Trial Investigators. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013 Dec 5;369(23):2197-206. [pubmed]
- Dankiewicz J, Cronberg T, Lilja G, Jakobsen JC, Levin H, Ullén S, Rylander C, Wise MP, Oddo M, Cariou A, Bělohlávek J, Hovdenes J, Saxena M, Kirkegaard H, Young PJ, Pelosi P, Storm C, Taccone FS, Joannidis M, Callaway C, Eastwood GM, Morgan MPG, Nordberg P, Erlinge D, Nichol AD, Chew MS, Hollenberg J, Thomas M, Bewley J, Sweet K, Grejs AM, Christensen S, Haenggi M, Levis A, Lundin A, Düring J, Schmidbauer S, Keeble TR, Karamasis GV, Schrag C, Faessler E, Smid O, Otáhal M, Maggiorini M, Wendel Garcia PD, Jaubert P, Cole JM, Solar M, Borgquist O, Leithner C, Abed-Maillard S, Navarra L, Annborn M, Undén J, Brunetti I, Awad A, McGuigan P, Bjørkholt Olsen R, Cassina T, Vignon P, Langeland H, Lange T, Friberg H, Nielsen N; TTM2 Trial Investigators. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N Engl J Med. 2021 Jun 17;384(24):2283-2294. [pubmed]


