Efficient and Effective Clinical Teaching
November 28, 2023
Teaching in the clinical environment can be… challenging. Learners are so enthusiastic, so engaged, and can require soooo much attention! In this podcast, we discuss ways to remain a kick-ass clinical educator and still have the time you need to be a, well, a clinician.
Efficient and Effective Clinical Teaching – The SimKit Podcast
Transcript
Hello everybody and welcome back to the SimKit podcast. Thank you for joining us today for our topic of teaching efficiently and effectively. Now, I first want to give a special thanks to Doctor Bob Trowbridge. He actually helped raise me as a clinician, was part of my medical education career and gave a fantastic talk on this topic, which I have borrowed and edited slightly.
So a couple of caveats to this conversation. This is of course, related to medical education. We’re talking about teaching efficiently and effectively for medical learners. We are really focusing here on the medical student. The approaches and techniques you’ll find probably don’t apply to more advanced learners like residents. But I do want to say that this can apply to a variety of medical learners- the learning nurse. It can apply to PA students and P students, nursing students, and they even can probably be used somewhat in your onboarding process if you are one of those people lucky enough to be involved in onboarding new trainees, you can use some of these techniques for that. So, it’s not exclusive to medical students, but we do want to apply the caveat that this is focusing primarily on those learners.
So I want to start by having you stop, think, pause- pause the recording if you have to- and just ask yourself, what are my individual barriers to being a good educator? I want you to actually to think out your answers. Think about the answers that you come up with for what your barriers are to educating these learners, particularly medical students, well.
Okay, hopefully you had a couple of moments to think about what your individual barriers are. But, I have a sense that some of them are going to fall into these four categories that are common for medical educators. One is that they can’t help me. Two, their presentations take too long. Three, they ask too many questions and the 4th is, which is kind of a, you know, bucket term for a lot of the problems that we inface as educators is there’s simply not enough time to teach. We’re going to tackle each one of these individually.
So first the idea that they can’t help me. I am a busy clinician. They are there to learn. They mostly get in my way and they don’t add anything to my clinical practice. Some of that may be true. Certainly, we don’t want to detract from the reality that working with a learner can interfere with your work environment and your efficiency. But the reality that they cannot help you, that is, that’s not a reality. That is a farce in my opinion. So to see how medical students and learners can indeed help you through the course of your day, ask yourself this first question, what are the time sucks in my day? What are things that take time away from my busy work environment that can be executed by some one of a technically, lower level of education or skill or technical needs in your clinic in your department that can be completed by them and there are many, many, many, many ones here. The list includes: doing a Med rec, updating problem lists, obtaining vital signs, obtaining old records, doing physical exam, calling and referrals, researching answers to clinical questions, doing patient education, and writing notes. All of these are elements that can be a time suck to our day. Which are incredibly valuable learning opportunities for a medical learner, particularly a medical student. So involving the learner in some of these elements, right? You’re about to go see a patient, it’s been a while since you saw them last. When the medical student goes in, ask them to do medric ask them to update problem lists. Have them do a set of vital signs. This is incredibly valuable for the learner but really could be a time suck for you and on the other side of things as you go through the end of the care of the patient, you can research a clinical question that you need to answer in real time. They can do some patient education on this, and they can even write notes to assist you in that capacity.
All right, #2, their presentations take too long. We all have seen it. We’ve all been there, the medical student presentation. In this, they go through the following process. They prep for the patient, they go and see the patient, they spend an exorbitant amount of time getting a history. Then they do a physical. They come out, think about things. Then they find us. They present the history, the physical exam, their differential diagnosis. You go in together with the patient. And the whole thing starts over again and you can feel yourself aging. You can feel the time being sucked out of your soul as you go through that process. This is an incredibly inefficient way to complete a medical student presentation, and there are many alternatives we’re going to talk about now. So to the dilemma of presentations taking too long, there are four solutions. #1 the bedside presentation, #2 bust into the exam room, #3 focusing the learner and #4 explicitly setting expectations. Going through each one individually, number one, that bedside presentation. In this, the student presents right in front of the patient. It is an opportunity for patient input and you can confirm findings at the same time. Now there are many, many myths about the bedside presentation. Three, we’re going to dissect now. Patients don’t like them. Preceptors don’t like them. Students don’t like them. Pretty straightforward. Let’s dive into each one. First myth: patients don’t like them. So this has actually been studied, and we’ll show you the references by Rodgers and Young. But when medical students or learners presented in front of the patient, they found that patients had a higher satisfaction with working with a learner. They found that there was a preference for bedside presentations in the future. There was no difference in confusion or discomfort. This comes back to the idea that a medical student might have a zebra diagnosis in their differential that you need to talk through, but oftentimes the patient may have the same concern. What if this is cancer, you know? I went on WebMD and the endpoint of course always is cancer. So by bringing these into the four, it’s often a patient question and it did not affect confusion or discomfort by the patient and they actually had an increased perception of time with the doctor, they felt that you spent more time with them. This is a magic trick, right? It’s like sitting down during examinations. 1.5 times increase perception of time spent with the provider. Same effect here. #2 preceptors don’t like them. In the Young study, they found that actually there is a higher perception of learner understanding which also was seen in the patient. There was a higher perception of patient understanding of the visit. They really appreciated the patient involvement in care and they felt like it actually enabled them to teach more effectively. Now, what about the third myth that learners don’t like them? Well, this one’s actually kind of a little bit, a little bit true. They found that initially learners in the Young study that learners were less comfortable in doing bedside presentations, but they did find that the more that learners were involved in them, the more they actually found, preferring bedside presentations. A lot of the reasons being the ones that we discussed above. So in summary, the bedside presentation is more efficient as we talked about all the time suck and you feel your age leaving you, your youth, leaving you as you hear a long, long winded medical student presentation. You can combat that by doing a bedside presentation, and there’s a lot of data to suggest that patients providers like them and learners learn to like them as well as they become more comfortable with them and eventually preferring them. All right, trick #2 for presentations taking too long. The bust into the exam room move. Sounds like a dance move, it is not. It is actually just a bit of a modification of the bedside presentation. In this, I love this technique because of our ability to do other things while the learner is involved in the patient care. The student starts with the patient. You do something else, and as a more efficient provider you could probably complete an entire other patient visit, analysis, examination, etcetera you do something else and then you bust into the patients room when you’re ready. This is great in that it one allows for direct observation of the student, both in history taking and physical exam skills. It allows you to do some modeling by you, the preceptor, and it gives you control of the visit length. No more 30-45 minutes for a scheduled 15 minute visit or in the emergency department visits that should be, you know, level 4, level 5, level, 3, should be fast and efficient. So to rehash that again a little bit as an example, you have two patients, Susan and David. They’re scheduled for different visit length. Susan has a 30 minute visit, David has 15. You let the students start with Susan and spend the 1st 15 minutes taking care of evaluating Susan. You complete the entirety of David’s 15 minute visit. When that is done and wrapped up, you bust into the exam room at the 15 minute mark. Involve yourself in Susan’s care. Get the summary and presentation from the patient and complete the patient visit. All right, onto the last two tricks for presentations taking too long, that is focusing the learner and explicitly setting expectations. I see these as two parts of the same tool. As an example, you know either you know repeat visit patients in the emergency department or in your clinic you got a visit with Chatty Kathy. We know Kathy is very verbose. She wants to spend a long time. She can consume your time with other patients. So in focusing the learner you say, like Chatty Kathy, I want you to focus directly on her diabetes control. This gives the learner the opportunity to work with very verbose and tangential patients, allows the learner to develop specific skills in redirecting the patient and focusing on the reason for visit or the chief complaint in the emergency department. And of course it offloads you. So by focusing the learner and setting explicit expectations you can narrow in on those very long patient visits. Alright, on to the next part of what learners do to suck time away from us and how we say they can’t help us. We say their presentations take too long. We talked about that. Number two. They ask too many questions. The key points here are to set expectations and we have to teach them to fish, right? You teach a person to fish and they can fish for a lifetime. In the first two solutions to this problem, we are going to be encouraging self-directed learning. When you complete a patient encounter with the learner, you’d ask them what about this patient interests you? You’re going to offer them the opportunity to build a question set related to that, and the second solution that builds off the 1st is using what are called educational prescriptions. You know the days of the old prescription pad sitting on your office desk are in the past are antiquated, but we all have small pieces of paper. You could have a pad or sticky notes that you can use in alternative. When you get a specific question from the learner after encouraging the self-directed learning, you give them the resource to answer it. You write the specific question on the pad and hand it to the learner. Very, very importantly, we are working with adult learners here. We don’t want them to feel like they’re wasting time. So of course we need to follow up their answer to that question. Either at the end of the day or the next time you work with the learner. Alright, the next two solutions to learners ask too many questions are the notebook and alternative learning experiences. So for the notebook, rather than having the learner ask questions ad hoc whenever they want related to patient care in the middle of the moment when you have a lot to do, you’re going to get a you know, bounded notebook. And they’re going to write down questions that they have that come up through the course of the day. At the end of the day, we’re going to review that list. We may find similarities/ differences we may have answered them through patient education. So some of these can be removed. At the end, when we aggregated all these questions, we can go back and again make our educational prescriptions and hand them to the learner. The 4th solution comes in what is called an alternative learning experiences. There are a few different ways that a learner can learn outside of being involved in your flow day-to-day. Moment to moment or in patient care. They can of course, prep for the next patient, they can work on schema related to disease processes or treatment algorithms and they can do structured reflection. So the first one, prepping for the next patient. That is relatively straightforward, in the emergency department, they sign up for the next patient, especially if they are complex or had recent care that needs to be reviewed. We can look at their medical history and prepare for them to evaluate that next person. In terms of researching and writing a schema, these are generally flow charts or infographics or diagrams on how to think about certain disease processes. Going through a work up for a patient or a treatment algorithm for them. There are a few different preconceived structures to do this. The Rational clinical exam and clinical problem solvers are two and you will find these references in the show notes. As an example, there are several structures and presentations or abnormalities that can be worked into a schema. Hyponatremia is a very common one. Trying to figure out are they hyper or hypovolemic? How does that affect it? Medications coming into play… There are many ways that they can create an algorithm and structure for thinking about this abnormality. Alright, the third trick in the alternative learning experience is a structured reflection. Structured reflections are a great way, especially when you’ve fallen quite behind for a learner to be involved and reflect on a patient care in a structured and meaningful way, while allowing you to do the work that you need to do. In these structured reflections, it’s usually a table that the learner fills in as they go. An example would be thinking about two or three things, conditions on the differential diagnosis for a patient. So if you have a patient with shortness of breath that you have seen together in the emergency department, they are going to put on their differential two or three things. CHF, COPD, pulmonary embolism, as example. Then they’re going to go through and list the aspects of the presentation that are concordant with the diagnosis of 1 area of the graph or table, and then aspects of the presentation that are discordant with the diagnosis. Finally, they’re going to list aspects of the presentation that are associated with the diagnosis, but we’re missing from that specific patient presentation. This allows them to really analytically think about the person presenting and the categories in which they can fit from a diagnostic standpoint, and again, it allows you to continue on with your day while they are still doing active and structured learning that you can critique at the end of the day or at another time. And the final one that we talked about, it was a bucket term. We don’t have enough time to teach by using these structures we outlined in the above, you are going to find yourself with more time, more energy and more structure to be enthusiastic about teaching your learners. So let’s go through things in order as a summary. When asking ourselves what are the barriers to allowing me to be a good clinical educator, there are generally three or four that come up. They can’t help me was 1. So we decided, let’s put them to work, recognize the things that are a time suck for you, but can add meaning for a learner early in their medical career. Allow them to do Med Recs, update problem lists, obtain vital signs, get old records, do physical exams, call referrals, research the answers to clinical questions, do patient education and write notes. The next, we said, is that their presentations take too long. They’re huge time suck. We talked about four ways to combat the hour long medical student presentation. One is bedside presentations, two is busted into the exam room, which is a modification of that bedside presentation where the learner works with the patient themselves and you come in at a time that’s convenient for you and three and four were to focus the learner and then explicitly set expectations for that patient visit and the information and physical exam you want the learner to do. The third and last was that they simply asked too many questions. We talked about how we need to run and set expectations that we want to answer all of their questions, and we need to find the right clinical time to do so. And then we recognize that we need to teach them the fish. We need to give them the resources and information so that they can answer their own clinical questions as part of their learning process. In doing so, we talked about encouraging self-directed learning. We talked about creating educational prescriptions where there is a question and a resource for them to answer and report back to you. We talked about the notebook effect or having a notebook available. This allows you to write down questions and keep them logged without having to stop your day in real time to answer each question the learner has. You then review them at the end of the day, remove ones that have been answered through patient education or other means, and can create educational prescriptions. And the fourth thing we talked about was alternative learning experiences. There are three that we saw here. They can prep for the next patient. They can build a schema related to an abnormality or other element of patient care they saw. And they could do a structured reflection. Again, these structured reflections on how to do them. We will give you some examples in our show notes.
So finally, if we think about the barriers we have in providing high quality education to our medical students and other early learners, we see problems in which we feel like they cannot help us set their presentations, take too long and they ask you many questions. You are now armed with a slew of ways of combating these barriers. Please take what information you find valuable from this, as well as the information again in the show notes to bring back to your clinical environment to give yourself the time to be a fantastic educator. Thanks so much for listening.
As you probably know by now, SimKit is very heavily dedicated to making procedural training fun and efficient. But these models and the training is not just for your own education. These simple, portable and easily accessible models can be used for interprofessional education, just in time teaching for medical students and residents, and so much more. Click the link on the bottom to learn more.
Practicing procedures can be tough. Let SimKit do all the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. We want you to be confident and competent clinicians, and we have the tools to help.
Efficient and Effective Clinical Teaching
First, let’s recognize that this podcast largely addressed these issues with being an educator of medical students. It is less applicable to learners further along in their training, like residents, who in their own right are often more advanced and “helpful” to the practicing doc. These principles do not apply just to the med student, but to NP and PA students, nursing students, and maybe even in the onboarding process of new grads – if you’re lucky enough to be involved in that process.
To frame this conversation, start by asking yourself:
What are my barriers to being a good clinical educator?
The Common Barriers
The most common barriers clinicians site for being a kick-ass clinical educator are the following:
- They can’t help me!
- Their presentations take too long!
- They ask too many questions!
- There is not enough time to teach!
We are going to address these first three concerns head on, and recognize the last one as a wastebasket reason that can be addressed by the first three.
#1 – They Can’t Help Me!
When addressing this first issue, it is helpful to do some internal reflection. This is done easily by asking yourself the following question:
What are the time-sucks in my day?
When doing this, we identify things you do that can be both educational to a new learner and liberating to you as a practicing clinician. These things include:
- Med recs
- Updating problem list
- Obtaining VS
- Obtaining old records
- Doing physical exam
- Calling referrals
- Researching answers to questions
- Doing patient education
- Writing notes
By giving these tasks to learners (medical students), they are given the opportunity to develop or hone a skill and you are given the opportunity to be more efficient.
#2 – Their Presentations Take Too Long!
We have all been on the receiving end of a medical student presentation. By the time they are done telling you the vocational history of their grandfather, you are ready to pull your freshly gray hair out! Think about the current structure of the medical student presentation. In this, they:
- Prep for the patient
- See the patient
- Get a history
- Do the physical
- Think about things
- Come out and find us
- Present the Hx, PE, DDx
- Go in together
- Start the whole thing over again
Is there anything more inefficient than this? Luckily, we have four solutions:
The Bedside Presentation
With this style, the student presents right in front of the patient! This gives the opportunity for patient input, and allows you to confirm findings along the way.
Now, there are a few myths about the Bedside Presentation that need debunking:
- Patients don’t like them- actually when this was studied head to head with the traditional presentation style [1, 2], they found higher patient satisfaction with learners, a preference for bedside presentations in the future, no increased confusion (the zebra diagnosis the med student brings up may very well be the patient’s concern), and increased perception of time with the preceptor.
- Preceptors don’t like them- again, when compared head to head with the traditional way [1], preceptors had a higher perception of learner and patient understanding, felt like patients were more involved in their care, and felt an increased ability to teach effectively.
- Learners don’t like them- Well, this one might be true, at least at first. Learners were seen to have initial discomfort with this presenting style, but the more they did it, the more they preferred this style over the traditional [1].
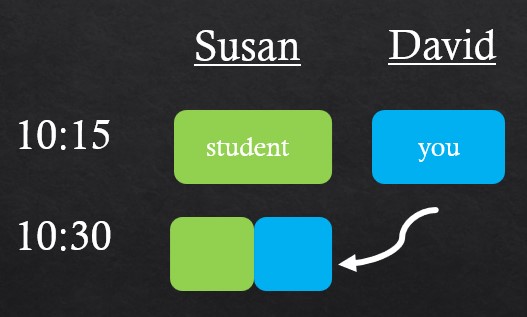
Bust Into the Exam Room
In this modification of the Bedside Presentation, you have the student start with the patient while you do something else (like complete an entire other patient encounter). When you are ready, you bust on in. This allows you to directly observe the medical student’s interaction with the patient, do some modeling as the preceptor, and importantly, control the visit length.
Below is a Bust Into the Exam Room example. In it, you complete a 15-minute encounter with David (maybe a lower acuity patient in the ED), while the student starts the 30-minute encounter with Susan. When you are ready, you bust on in, have the student present where they are at, and complete the encounter.
Focus The Learner And Explicitly Set Expectations
Tricks 3 and 4 work together. In them, you assist in focusing the learner on a goal of the encounter (ex: push them to the chief complain and not the 10 other, longstanding issues) and explicitly set expectations (ex: the patient’s chief complaint is chest pain. In 15 minutes I want you to get the PQRST historical elements of that pain, I’ll be with you after I finish up our patient with ankle sprain).
These tricks help the learner develop skills in working with very verbose and tangential patients, a commonality in all of medicine. It also offloads you!
#3 – They Ask Too Many Questions!
Having an engaged and enthusiastic learner is a blessing…. and a curse. The curse is that all their questions can eat up your clinical time. The first reality is that we have to set expectations. Letting the learner know their questions are important to us, but have to be addressed while still providing care is important. Secondly, we have to teach them to fish. Meaning we have to give them the skills to catalog and answer some of their own questions. This is something we all still (hopefully) do, so is a lifelong skill to learn. To specifically address the learner that asks lots of questions, we again have 4 solutions.
Encourage Self Directed Learning
Here, we engage the learner. Ask them “what about this patient interests you?” Then, we encourage them to build a question set around this patient and their presentation.
Build Educational Prescriptions
Once we have our questions from the encounter (above), we write an educational prescription. Now, the days of prescription pads lying around ERs and offices are over, but sticky notes and scrap paper serve the same purpose. Get a specific question from the learner, write it down, and give them one or two resources for finding the answer. Very importantly, don’t forget to follow up with them on the answers they found!
The Notebook
With this trick, you or the learner have a standard, old school notebook that you catalog questions in to be answered at a later time. At the end of the day or shift, you review these questions. Amazingly, many of them will be answered through patient education or other clinical work! In the ones that remain, write out educational prescriptions for the learner and review them after some independent learning.
Alternative Learning Experiences
For the learner that asks a lot of questions, you may simply need to unload/unburden yourself. You can do this in three ways:
1. Prep for the Next Patient – Have the learner occupy themselves in preparation for the next patient by reviewing problem lists, prior encounters, and current medications.
2. Build Schema – Schema are frameworks for organizing and thinking about symptoms and medical conditions (ex: causes of hyponatremia). They often come in the form of infographics and algorithms. There are several resources for helping a student identify or build a schema. Two great ones are:
3. Structured Reflection – In this, the learner identifies 2 or 3 items on the patient’s Differential Diagnosis and thinks critically about what in the patient’s story or physical exam fits, what doesn’t fit, and what is missing. Below is a document for a structured reflection. Feel free to download and print this out for use in your clinical setting.
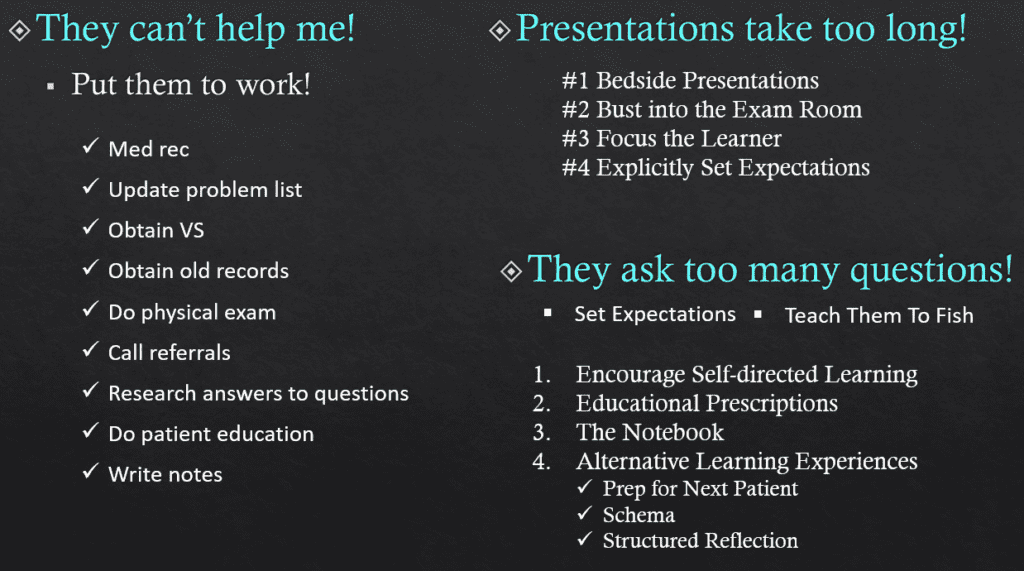
Summary
In many ways, having learners is a Godsend for clinicians. They invigorate us, challenging us, and keep us sharp. But teaching as a clinician has its challenges. Below is a graphic depiction of the common challenges we face as clinical educators, and how to combat them. Feel free to download and save this to your peripheral brain (i.e. EverNote) to reference the next time your on shift.
See more on the topic from the great Emergency Medicine Cases podcast!

References
- Young L, Rego P, Peterson R. Clinical location and student learning: outcomes from the LCAP program in Queensland, Australia. Teach Learn Med. 2008 Jul-Sep;20(3):261-6. [pubmed]
- Rogers HD, Carline JD, Paauw DS. Examination room presentations in general internal medicine clinic: patients’ and students’ perceptions. Acad Med. 2003 Sep;78(9):945-9. doi: 10.1097/00001888-200309000-00023. PMID: 14507630. [pubmed]
- Regan-Smith M, Young WW, Keller AM. An efficient and effective teaching model for ambulatory education. Acad Med. 2002 Jul;77(7):593-9. [pubmed]
- Usatine RP, Tremoulet PT, Irby D. Time-efficient preceptors in ambulatory care settings. Acad Med. 2000 Jun;75(6):639-42. [pubmed]
- DeWitt DE. Incorporating medical students into your practice. Aust Fam Physician. 2006 Jan-Feb;35(1-2):24-6. PMID: 16489381. [pubmed]
- McGee SR, Irby DM. Teaching in the outpatient clinic. Practical tips. J Gen Intern Med. 1997 Apr;12 Suppl 2(Suppl 2):S34-40. [pubmed]
- Dobbie AE, Tysinger JW, Freeman J. Strategies for efficient office precepting. Fam Med. 2005 Apr;37(4):239-41. PMID: 15812687. [pubmed]


