Under the Skin: A Necrotizing Fasciitis Story
Contributor: Jason Hine MD and Shawn Stepp PA
In our latest episode of the SimKit podcast, we dive into a riveting discussion with physician assistant (PA) extraordinaire, Shawn Stepp, to delve into a complicated case of necrotizing fasciitis. This post breaks down the conversation into five key sections, each shedding light on different aspects of this challenging medical condition.
Transcript
+
Alright. Hello everybody. Hello, hello and welcome back. Welcome back to the Sim Kitt podcast. I am here. I’m joined today by a special guest for me. It’s always fun when you get to bring in a colleague and I’m joined by Shawn Step. He’s a PA extraordinaire who I have had the pleasure of working with for.
Just shy of a decade, Shawn?
Something like that. Yeah, a long time now.
Been a good little while. Been a minute. As I say in New York or Philly. Depends. That’s a minute In Philly is a long time. A minute in New York is a second, but we’ve been working together for a while and we’re here to talk about an interesting case that Shawn had.
And so Shawn, thank you so much for joining us and tell the listeners a little bit about yourself.
Yeah, so I’m a pa. I’ve been doing emergency medicine for about, uh. 14 years now and it’s, uh, yeah, become where I’ve landed and, uh, very much enjoy it. So, grew up in Pittsburgh and now up in the northeast.
Excellent. Well, thanks for joining us again and let’s, let’s get into the case. Tell us, just kind of paint us a picture, if you will, Shawn, tell us what brought the patient into the er, maybe what the triage was like. Give, give us a little bit of background for the case.
Absolutely. So I actually have the triage note here, and this is a 40 ish year old male, um, who is ambulatory to triage with an what he complains of an infected right foot wound for 40 days.
Uh, told the nurse, he broke the foot 40 days ago in Italy and was not given a cast. And then at some point there was a blister. At some point he took amoxicillin, uh, pretty vague on the details. He put a corn remover tab on it and he, uh, comes in. Saying that now he’s just not feeling so good after the last, over the last kind of 24 hours.
Hmm, okay.
Um, and the, yeah. And the, uh, triage nurse notes that he looks kind of clammy. Clammy. And that was, uh, that was the note. Just to
clarify that. 4 0 4 D four zero days of a
yes. Yeah. Huh. And 40 days. That’s, that’s, that was his initial report. Okay. A little more clarification as it goes.
Yeah. As, as they always do, you just peel back the layers of the onion and it gets more wild.
Um, all right. So 40 ish, year old male, 40 days of an infection and just not feeling great. All right. Right. Um, okay. Triage vitals. Uh, what’d they look like?
Yeah, so 36.6 degrees Celsius. Heart rate was 100 to one 10. Blood pressure was 96 over 51. Respiratory rate, 16 O2 saturation, 95%. So obviously a couple things stick out there.
Yeah. Yeah. Okay. So high heart rate, little bit soft pressure. Okay. Okay. And then, uh, a fever,
interestingly.
Yeah, no fever, right? Yep. And then what was kinda, what was the look from the door? You know, the, there’s sometimes you can tell a, a whole story just by entering a room.
Yeah. I walk in and he doesn’t look good.
Um, you know, and he’s not like. He’s clammy, he looks pale. Um, he’s not diaphoretic necessarily, but, um, he just, he looks ill. Okay. That was my initial, you know, across the room. Like, this guy doesn’t look good at all. Yeah, I gotcha.
And you’re sick, not sick. You’re putting him in the sick camp or at least feelers out that something’s not right.
Yeah, something’s not right. Yeah, for sure.
And then sort of go through, if you would, uh, keep going with your story as you kind of get into the room, dive into details, tell us how this progresses.
Yeah. So he’s very dismissive of his symptoms. He’s like, yeah, I think it’s a little infected. I think it might need, you know, maybe a little work.
That’s kind of how he put it. He said he has his foot wrapped in a bunch of gauze really tightly. Um, and he’s kind of vague about his symptoms, but he, you know, he kind of tells me a few times as I walk in, I just want some treatment and then maybe some antibiotics I know I need, need to go home. Um, but he’s like, you really don’t wanna unwrap it ’cause it smells.
And I’m like, well. I’m gonna have to unwrap it, especially if it really smells. Um, so that was kind of our, our initial interaction. But then I was able to kind of get him talking a little bit more. And so here’s a little bit further history. Um, he says that he broke his foot in Italy about one to two months ago.
He says he just twisted it. It was a mechanical fall. I didn’t think it was a big deal. Went to, um, some sort of walk-in there, had x-rays and there was a fracture. And he said they, they told him he actually didn’t need to have a cast. He said he should probably be off it for a couple days, but for his work, he said he couldn’t be, he had to go out and walk and he walked like nine or 10 miles the day after he broke it in a walking boot.
Okay.
Um, when I ask him where he broke it, uh, he points to the fifth metatarsal area. Um. He said a few weeks after he broke it, um, he saw a blister in the area and he thinks because it got wet from walking out in the rain one day.
Hmm.
Um, and so he started putting a bag on it, is what he said. Um, and so a, a few weeks after he broke it with the blister, he went and was seen again.
Um, they repeated x-rays at the time, according to him, and it was, uh, healing well. They placed him on antibiotics. He remembered that he was placed on amoxicillin and something for MRSA. Um, but he couldn’t remember the name of the antibiotic that he was placed on for MRSA. Um, he came back from Italy. Uh, little vague exactly when he came back.
I eventually found out from his mom that he came back about, uh, three and a half weeks prior to he presented to the emergency department. Okay. And he’d been off of antibiotics for, uh, at least a week. Uh, maybe more the little corn tav remover. He said that he then developed like this hardened kind of painful spot now at the base of the great toe.
And so he thought maybe it was a corn. And so he put that on there and then that opened up and became kind of blistered and became a wound as well, two days before he arrived.
Hmm. And
then over the last one to two days, he stated that it really started to smell, um, and it started really just draining copious amounts of fluid.
And, uh, that’s the two wounds have a blackish appearance at the base of them, and he just started to kind of just feel tired. Okay. That is a wild story. Interestingly. Doesn’t mention story, isn’t it? Isn’t it crazy? Yeah. Interestingly, did not mention pain was very, um, kind of dismissive of how sick he may be.
Okay. Um, very interesting.
Yeah. And then another thing jumps out at me, so a few things are going through my head as you tell me the story. I was thinking maybe an avulsion of the lateral malleolus, something that you can walk on then pointing to the foot. Okay, so hopefully this wasn’t a Jones or a stress, maybe it’s a pseudo Jones.
Something like that could be. Ambulatory. Um, but then big thing, big, big, big jump point, uh, you mentioned a mother and so yeah, collateral. When you’re just like, what is go, what is going on here? What is your ability to relate a story? How much can I trust? The history I’m getting. What’s mom’s take in the room?
What is, what is the engagement, you know, eye rolling and corrections a lot, or collaboration, kind of how’s that dynamic?
Yeah, great question. So she showed up about 10 to 15 minutes after I first saw him and was able to get, so he had already been over to X-ray. I was actually just, I brought in, you know, I was walking in to look at the X-ray with them when, uh, she showed up.
Um, so yeah. She was extremely concerned. Apparently she’d been trying to get him to be seen for the past three weeks, um, and felt like he was much sicker than he was letting on and was downplaying his symptoms. Gotcha.
Okay. Okay. And then I’m gonna do, I guess a little like mini oral board style stuff, just to get a little bit more of the story and, uh, foundational things.
So, uh, are, is this individual in our health system. Do we have records? No,
we have no records on ’em.
Lovely. And, and asking the, the person, the me, the patient, past medical history, what do we
gather? He denies everything. He says that he is a healthy 40 ish male. Doesn’t see doctors, hadn’t seen a doctor in a long time.
Um, and he denies a history of diabetes to me.
Yep. Yeah, that’ll come into play certainly. And then social stuff we’re gonna want to know about, uh, eventually, but. Yeah, it is great when you don’t have medical history or don’t have medical problems. Um, I always find that the immediate follow up question has to be, you’re healthy, you have no medical conditions.
When was the last time you saw a doctor? ’cause right. Obviously many of those are just under or un undiagnosed. So yeah. Hasn’t seen a doctor for a long time. We have no baseline, uh, medical conditions known. Okay. Um, get, let’s get into the physical exam a little bit, uh, for me, if you like. Sure.
Yeah. Again, you know, he’s clammy.
He doesn’t look well, and then when I unwrap his foot, it is, uh, quite smelly. Like to the point that, you know, I’d already brought a mask in, but I was very happy I had it. Mm-hmm. Um, and looking at his wounds, um, of the right foot, um, just kind of go to really where things were over the kind of distal first.
Um. Me metatarsal. So kind of that, uh, at the base of the great toe
mm-hmm.
There is this, uh, blackened area from the planter aspect of the toe. Through that kind of distal first metatarsal, it measures about 10 by five centimeters. Uh, so, and it’s weeping, just a copious amount of serous fluid. Doesn’t really look initially purulent, which was interesting, but I mean, just dripping yellow, serous, um, foul smelling fluid.
Okay. Very malodorous. Okay.
Yeah. And there’s kind of significant sloughing of the skin, that kind of macerated skin all around the wound. And, um, then it almost looks like the skin, honestly, if I pulled on it on that great toe would just come right off. Um, it would completely deglove the toe. The, then there’s a similar, somewhat similar appearing wound of the lateral aspect of the foot over the line distal fifth metatarsal.
And it measures about five centimeters in diameter. It’s also kind of black at, uh, at the base of the wound. Um, certainly can see all the way through to, um, soft tissue there. He did not seem to have much pain, so I actually used a Q-tip and it did seem to probe to, you know, something hard eventually.
Mm-hmm. Um.
And this is, again, surrounded by some edema and, uh, a little bit of macerated skin, but not nearly as much as was of the great toe. And it was also kind of draining, copious, serous fluid. And then there’s really, you know, interestingly, the, the rest of the foot is erythematous, but kind of subtle.
It’s not like that really bright erythema. Um, it wasn’t like super underrated. It was maybe a little bit. You would expect, um, with a cellulitis. There was, there was, but it was subtle. Erythema. Erythema. Um, and it was darker on the foot itself. And then above the ankle. It was very kind of light all the way up to the tibial plateau.
And it, yeah, and it felt really boggy and there was edema associated with a, with a kind of subtle everything, but it’s again, very subtle. Um, it felt boggy, not like super underrated, interestingly. Um, and as I’m feeling it, I’m like. Man, this, I think there might be air underneath the skin here, um, especially of the foot and of the anterior, uh, lower leg.
Um, so I’m, I, you know, became concerned about crepitus obviously, so. Sure. Okay.
Uh, tell me about the vascular exam. Could you feel a DP or P.
Yes, I could. It was subtle, but it was certainly there. So DP and PT were both present. Were present. Okay.
And then in palpation and, um, that area of inspection, what was the patient’s engagement or reaction to you, allowing you to touch, allowing you to squeeze, not.
Yeah, so he certainly had some tenderness. You know, he’s denying that it really hurts, um, to me in history, but he certainly had tenderness. Um, it was, it was somewhat painful, but it wasn’t exquisitely, and he certainly wasn’t in nearly as much pain as I would expect as. For someone who looks like his toe was almost falling off.
I mean Yeah. You know, he was downplaying all his symptoms. Certainly didn’t want anything for pain. It’s just kind of mildly tender to him. Um, so certainly it wasn’t, um, you know, it, it was almost the opposite of what I had ex I expected when it came to pain. Sure.
Okay. And so coming out of the room, there are a couple big, obviously one huge red flag in there.
Um, that. Maybe focuses are differential, but what were your, what was your differential and what were your orders after that exam?
Yeah, so I mean I did the big sepsis protocol obviously. Um, and then, you know, as far as the actual type of infection, this is obviously a deeper, you know, with the time course, initially I was, when he first was telling me about it, I was thinking maybe about, maybe a chronic osteomyelitis.
Mm-hmm. That
maybe then has developed more of an acute. Side of it, you know, kind of an acute on chronic type of type of picture. Um, but then with the crepitus now I’m thinking, okay, gasping green or, uh, necrotizing fasciitis, or some sort of combination between all two, uh, you know, all three of those, you know?
Uh, so this is kind of my, uh, major concern at this point. I went ahead and paged burn soft tissue.
Okay. So you did immediately out of the room and
outside? No, I, yeah. Yeah, I, yeah, I guess I should clarify. I ordered, I ordered everything, including x-ray and I said, let’s get this x-ray done right now. Mm-hmm.
And
went ahead and paged, uh, as the x-ray was being done.
Yeah, when you start having that question of that crepitus, um, you know, vital signs, we, we kind of didn’t brush over them, but we noted a soft BP and elevated heart rate. Um, and then we order our sepsis order set. We’ll go through a little bit more of the specifics there in a minute.
Uh, you, you have concern for repi. You get an X-ray ordered and you page immediately, so, fantastic. Um, differential, I’m gonna consolidate it a little bit, starting at cellulitis. Um, it sounds like with the vascular exam, you know, ischemic. Slim is less likely. Right. But that’s certainly something that you would keep on your differential with someone who has Sure.
Basically soft swathing soft tissue, um, osteomyelitis with a blossoming, um, soft tissue infection around it with a time course. I would keep in there even, you know, abscess formation or something that’s not responded to his amoxicillin Plus whatever MRSA antibiotic he was on. But I mean, let’s call s spade a spade.
When you start feeling or concern that there’s crappiness in the soft tissue, we have neck, fa, neck, fa, neck, fa as our, as our top three. Right? So, awesome. Alright. And so what did you order, um, in terms of therapeutics?
Yeah, so initially with the sepsis protocol, it was cine vancomycin, and then I added on clindamycin.
Um, so we, we kind of started there, um, until I talked to burning soft tissue.
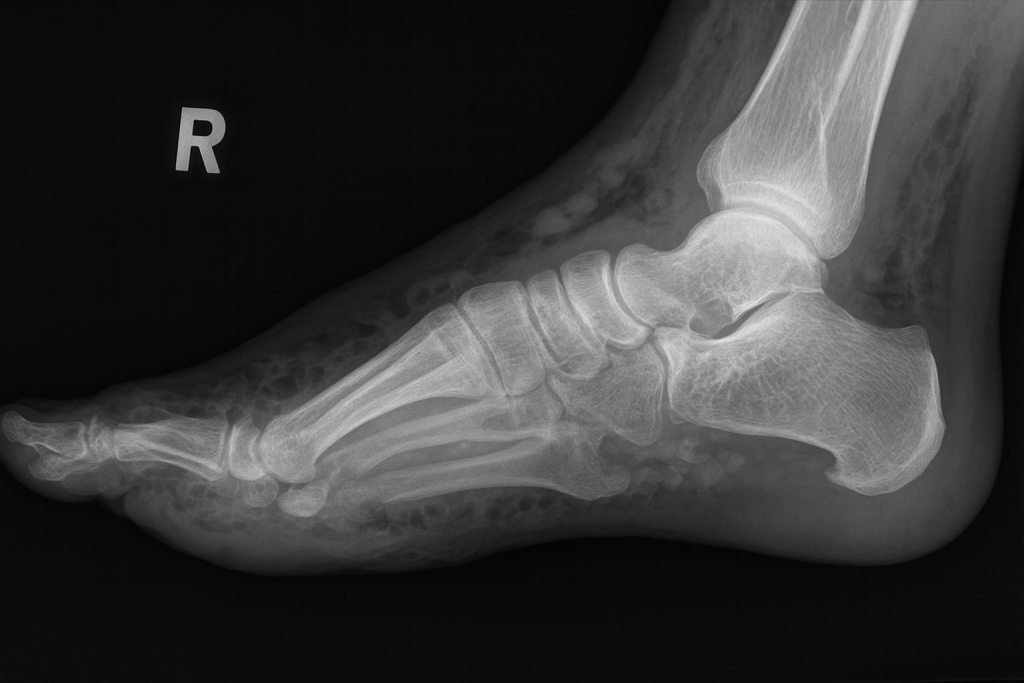
Okay, great, great. And, um, was the x-ray confirmatory or what did it show in terms of, in increasing or decreasing your concerns for neck vash?
Yeah, so the x-ray was quite concerning. There was, um, bony erosions of the fifth metatarsal.
Essentially the entire head was gone and the, uh, the proximal and, you know, the, the failings were gone too. And then of the, uh, first. You know, the great toe.
Mm-hmm.
The both, the phalanxes were pretty, um, pretty significant bony erosions and some of the first metatarsal head as well. And then I could see gas.
I could see gas in a soft tissue on the x-ray of the foot. Um, and so yeah, obviously that confirmed what I thought was maybe crepitus, you know, I wasn’t sure to be honest with you. I was like, well probably. Um, but you know, the x-ray was certainly concerning. Gotcha. So it was there
on x-ray. Okay. Yeah. And, um, I guess, what was your thought process?
If that x-ray was negative, where would you have gone from there?
Yeah, that’s a good question. You know, because he, it, it wa you know, ’cause mom wasn’t here yet and he was certainly downplaying everything. So, you know, I would hope that would’ve gone the same direction at least. And, you know, continued with the consult.
Um. And you know what? The consult, when I talked to Burn soft tissue, what they wanted me to get was, you know, immediately send ’em up. You know, because we, we don’t have, uh, those resources where in our current emergency department, so
mm-hmm.
Um, to send ’em up to the tertiary care center, but also, um, they wanted a, you know, quick CT non-con, uh, of the leg and then just load ’em up and send them.
So I would hope I would’ve gone that same direction. But, um, you know, if I didn’t see it, um. On the x-ray, um, hopefully I would’ve just gone right to the CT and continued to consult ’cause he was certainly concerning enough on exam.
Yeah. Yeah. And so, um, let’s go over some of the lab tests and that may even further drive some of that, you know, post-test probability, right?
Your, your x-ray and you’re chasing the next imaging. Sure. Depend on the patient’s global clinical picture. So, uh, yeah, what was the, what’d you find in labs? What, where did things go? Yeah,
so labs started rolling in as, uh, burn soft tissue. Called me back. And yeah, his leukocytes were 41,000. Um, hemoglobin was 9.2.
Uh, obviously with leukocytes he had quite the left shift, 89% neutrophils. Lactate was 3.5. CRP was 2 68. Um, his sodium was 1 28. Uh, chloride 93, uh, creatinine 1.57. And, uh, and that’s in milligrams per deciliter. And his glucose was two 60. Um, so certainly significant across the board.
Yeah. And those are without priors, I’m assuming, right?
Yeah.
Nothing to compare it to. Okay. Oh said rate was 62 too. That came back later, but,
okay. Um, remarkable. CRP, um, a notable, well say that glucose again.
Glucose was two 60. Yeah, two 60.
Okay. Okay. Yeah. I’m gonna get guess that there’s an anion gap, both from probably the sugar. You know,
interestingly, it was right on the top end.
Um, it was right at 16.
Yeah,
isn’t that tracking? Um, yeah, so right on the, on the top end there. Yeah. I wonder what his counter
regulatory alkalosis would be from, but interesting. Yeah. So you’re seeing probably an acute kidney injury. You know, he is 1.57, I think he said he’s got, you know, unrecognized diabetes, um, he’s got hyponatremia.
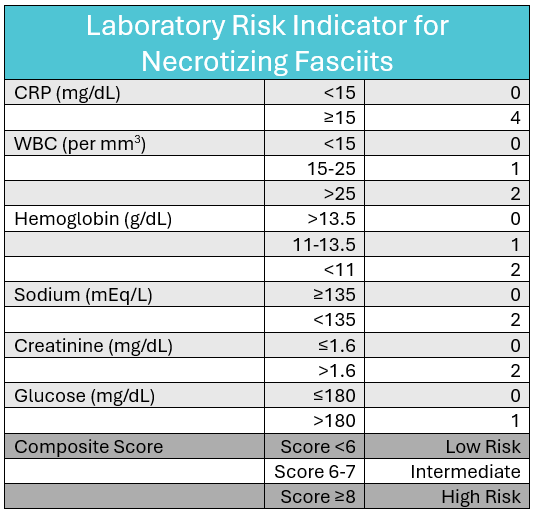
So did the, lrinec score, uh, did that pop into your head? Or is there a calculation? Obviously you had a slam dunk on your x-ray, so maybe not, but what, right in your brain?
Yeah, so I remember that there was a scoring system. Um, I didn’t use it in the moment because, you know, I was already, you know, kind of going down that road.
Um, yeah. But, um, when I did, I looked it up later just to kind of plug in. His numbers and Yeah, of course he, you know, it’s, it’s the, the hyponatremia, the acute kidney injury, the elevated glucose is actually a part of it. Um, the anemia, the lactate, the CRP, the elevated, you know, leukocytes. So he basically was, you know, according to the scoring, uh, you know, it was very, uh, specific for necrotizing fasciitis, most likely.
Yeah. He hits those numbers. I think his, he actually doesn’t get, just barely, doesn’t get scored on creatinine, but, so this, I, pronunciation wise, go back real quick. So it is a, a laboratory risk indicator for necrotizing fasciitis, which is, we’ll dive into the details of it. You know, it’s a non-specific test.
It doesn’t have amazing characteristics, but it’s assistive. Right? Um, yeah. And it’s like, you know, if you have a ultrasound showing appendicitis, you don’t need to do a pediatric appendicitis risk score. Um, when you have gas cracking up a leg, it doesn’t make sense for you to be doing that score calculation.
So yeah, it makes sense that it’s there, it’s recognized. Um, but I think. And we’ll put in the show notes. The elements that I, I think are important, you know, whether or not the score itself can be, uh, relied upon, which it cannot. Um, the parts of it that highlight, uh, for me are really the markedly elevated CRP.
So you get a lot of your points in the CRP, and then when I start seeing the hyponatremia, acute kidney injury. With a high CRP, that, that’s kind of like, that’s the important thing in my brain, um, to keep in mind. So, uh, we don’t go through social on this, gentlemen. I don’t know if there’s a lot in there.
Sounds like we had an unrecognized or undiagnosed diabetes as is probable precipitant or, um, risk factor. Um, unless there’s a, you know, IVDU history as well, homelessness, um, and alcohol or other ones that we consider, but, um, I don’t think that. In that real time in the story that you’re painting is necessary to get all of those risk factors out of this particular individual?
Yeah. Yeah. I mean, what I was able to get is, you know, I didn’t think there was significant alcohol history. I certainly put on an alcohol level, which was zero. Um, and he, he denied a significant history. Um, he denied being homeless, but was very vague about his, uh, you know, what he was doing walking around Europe.
Um, so yeah, so that’s kind of where we were. Okay.
That’s an interesting case. And so, uh, play out that rest. So you get your x-ray, you see gas, you have burn soft tissue, they want non-con ct, right? Quick, kind of how did it go from there?
Yeah, so, you know, as soon as the CT scan was done, we had the ambulance, you know, ready to roll for him.
Thankfully we had an ambulance right there and got ’em loaded up and out the door. Um, so. For him and his, you know, his ANA box was still running at that time and I kind of prepped him as best I could that he was likely going to lose at least a portion of the leg. Um, and, you know, this was quite obviously shocking for him, but he, it was interesting that he was then able to give me more specific history.
Um, you know, so a lot of that history I gave you kind of came after I said, Hey. You’re probably gonna lose at least a portion of this leg. And then it kind of like, it was, it was interesting. He was then able to kind of give me more specifics. Well, it was two weeks ago when I was on this, you know? Mm-hmm.
And, um, so yeah, he ended up with a, um, below knee amputation. Um, they tried, you know, they, they explored some of the soft tissue initially in the surgery and it was just, basically it was necrotic everywhere. It’s gone. Yeah. Um, down to the muscle. And, um, so they ended up needing to do a blow knee amputation and he continued to have, uh, continued soft tissue infection at the site.
And so he actually ended up with an above knee amputation eventually. Um, so he. He eventually did tell staff at the hospital that he, um, was diagnosed with diabetes in 2016 and was placed on Metformin, but he exercised and lost weight and his hemoglobin A1C normalized and so had been off of metformin, but then also hadn’t seen a doctor since probably 2017, 2018.
Okay.
Um, yeah, so BACE Globin A1C was 7.2 during the hospital stay. So not, not terrible. Yeah. Um, blood cultures were negative. Uh, so interestingly, and the wound culture, uh, displayed Proteus miis as the primary. Um, you know, I did, I did wound cultures there. You know, it’s probably very polymicrobial. There’s also some streptococcus species in there, or will not group a strep.
Um, but probably streptococcus, aosis. Um, but they were like, that’s, that’s, that’s obviously on the skin a lot of the time, so probably not creating an infection, but who knows? Um, but definitely, definitely Proteus in the wound.
Okay. Well, so
yeah, so it was interesting,
but I think the thing that you, you glazed over, which you shouldn’t and you should get kudos for, um, is he, the first thing you said is he is, he had, and he continued to have and these things, and he’s alive.
Yeah, like the, the, the patient survived the disease process. Yes. He’s
doing very well.
Yeah. And no longer, you know, be above knee. Um, and he kind of plays out perfectly, minus a couple parts. So, so let’s, let’s kind of like dissect the case, but the fact that the individual survived. Uh, great job, Shawn. That’s f.
Um, so the biggest thing for me that is like, just completely discordant with what we teach, what we know is the lack of pain, right? Yeah. So yes, scoop pain out of proportion. That’s kind of like the bread and butter things that make us first start getting air, getting our feelers for neck, right? Um, and we didn’t have that.
And I remember the reason why I wanted to bring you on the podcast, one, because it was a great case and a kind of a delayed presentation of a serious illness that the patient survived. And two, uh, just to talk about that, like label and deferrals, whether or not this is actually. LA be De France is, is probably an area of question, um, globally, you know, that is more of a psychiatric condition, right?
We talk about La belle indifferance in terms of like conversion disorder. People that are like, yeah, no, I can’t see. And I haven’t been able to see for the last like, you know, 45 minutes and they just simply don’t care. Um, but this type of LaBelle Defra is probably. In the fact that, you know, his disease process was tracking all the way up into the lower tibial region.
Right? Right. And so this is a physiologic, um, lab Deron, and that he probably had pretty severe pain. Maybe he had some unrecognized peripheral neuropathy, but then the disease process killed all his nerves. Right. And that he lost that sensation, which is interesting.
Right, right. I mean, he could still move the foot.
He still had some sensation. Yeah. But denied significant pain, which was Yeah. Yeah, very. And he was very dismissive. Um. Again, you know, who knows if that’s his personality per se. Mm-hmm. But, um, it did make the initial diagnosis a little bit difficult until I took the wraps off his foot. I’m glad
you didn’t listen to ’em and that you took the off.
Yeah. Yeah. Um, all right, well let’s get into some teaching points for neck fash. Uh, so this is more common in kind of the middle age or the elderly. You know, I’m, I’m coming up on my 40th, so I don’t know if I’d say mid forties is elderly, but, uh, middle aged, Hey, hey, it fits for me. No.
Yeah,
there you go. Um, and diabetes, you know, diabetes, I, I think of as my, my most common or most prominent risk factor.
You know, people that have peripheral vascular disease obviously are gonna be, those are kindred spirits in a lot of way, uh, in terms of microvascular disease or lower extremity, um, you know, flow limitations. But peripheral vascular disease can be another. Risk factor we talked about, um, you know, cirrhosis and um, IVDU.
Um, those elements coming into play, uh, immunocompromised state, homeless state, those are all things that could be, you know, more likely to lead to a necrotizing fasciitis infection, but. The scary part is, you know, I think it’s a third, 25%, 33%, somewhere in that space can happen in pretty healthy, uh, individuals otherwise, uh, which is kind of, kind of crazy.
And that, that breaks down into the three types, right? I, I think of the, kind of right down the fairway, the one that I think we probably see the most is the type one that polymicrobial in the diabetes patients, um, older patients, and then the, that. One that scares me that kind of like 25% are a little bit greater.
The healthy people, that’s the type two where the younger people happens, maybe after a burn, maybe after trauma. Um, and then type three, that’s that like board exam, cirrhotic patient who eats vibrio, basically it’s oysters and gets Vibrio. Uh. So a marine exposure or water exposure, someone with liver disease who can develop that type of infection.
Yeah. Um, so pretty interesting, the three types. It sounds like this gentleman had the polymicrobial type one.
Yeah. Yeah, I think so. Even though he was from a kind of, you know, I’m 46, right. So he is gotta be in the type two, but now Yeah. But yeah, no, probably type one. Yeah. Yeah. And remind me of the pathogen.
Are there multiple. It was, well, protease, MIVAL is what, uh, you know, grew out primarily. Um, and I, that was just me taking a wound culture. Um, the, there was a streptococcus, um, species, but not group a, not one that would typically cause infection that, you know, can often live on our skin. It was, uh, I have to look back here, but I assume it was streptococcus and gen.
Okay. Uh, yeah, an gens. Okay.
Wow.
Yeah. Interesting. Um, all right. And then, so other teaching points, we talked a little bit about 📍 the lair nick score, the L-L-R-I-N-E-C score. Um, you know, sensitivity is not great. 60, 70%. Um, you know, so it’s, it can’t be relied upon really to rule in or rule out. Um, the specificity is not perfect either, but I think the components.
Are the important part, right? The they, it doesn’t have a, it’s all laboratory. The L is for laboratory, so that’s. An important caveat. You know, it’s not gonna include paid out of proportion. It’s not gonna include risk factors a patient might have, but when you start seeing those like crazy CRPS and the acute kidney injury, and particularly the hyponatremia that really starts make, you know, starts to make me think obviously about systemic illness.
Um, sure. More so than like a simple cellulitis. But, uh, I think if you take the components, which will include in the show notes and include those into your thought process when you see. A sicker than typical lytic patient. That’s kind of where that plays out for me.
Yeah. Yep. Yeah, for sure.
What was the sodium on that guy?
Remind me. It
was, yeah. One 20 something. One i one 20 is, lemme scrap the action. 1 28.
1 28. Yeah. And so they’re talking about numbers less than, uh, 1 35 here. And we’ll again, include this in the show notes. Um, so imaging, you know, I’m, I’m happy that it was a clean. Diagdiagnosis off of x-ray and it speaks to the advanced disease, right?
Um, and the fact that the individual survived despite advanced disease. That’s impressive on that person’s accord. Um, because time is our biggest problem in terms of delayed diagnosis. You know, about three quarters of these are gonna be diagnosed as cellulitis. The first time until they get sicker. Um, so imaging nice to be able to see it on x-ray.
Um, other things you can utilize is if you’re, you know, ultrasound savvy, you can find that subq gas ideally. Um, but CT to the point of the, uh, burns soft tissue people, I think they probably wanted to see how far up the fascial planes the edema was and how exactly high the um. The gas was spreading. Uh, so they can know where their margins are gonna be when they go in for surgery, but that’s the most easily accessible and probably helpful in our areas of delineating those fascial edema and things like that.
Um, the sad thing is that none of the above really can. Be relied upon. None of them are, are things you can hang your hat on. Right, right. I start seeing edema up a fascial plane, well, above your area of moderate cellulitis, then you’re pointing yourself in that direction, but none of these are perfect.
Yeah. And just, you know, these amount of bacteria don’t produce gas, so
Yeah. Yeah. Right. Can’t rely on
that either.
Exactly. That’s, that’s a pretty scary part. Like we talk about the clostridial species classically. Being the gas farmers. Um, so I’m wondering what, you know, in that polymicrobial for this guy was producing the gas, which really sure.
Saved him maybe in its own right. Got him to where you could see it. We could find out what his illness was, um, and get him to the OR quickly. But yeah, so x-ray, CT, ultrasound, great. If they’re positive. Not if they aren’t basically, which is a theme. All of this is a theme, like no physical exam finding, no specific lab, no specific imaging.
It’s the whole, the whole, uh, test together. I thought it was super interesting when you just started to describe the discharge. ’cause like it wasn’t really purulent, it was kind of ous. It was very malodorous. And I’m like, that’s like dish was the, the gray dish Water discharge. Yeah. Sink. Yeah. That’s kind of what
it was.
Yeah, exactly. Kind of serous, yellowish gray. Yeah.
Yeah. Which is, um, another, you know, as we’re thinking about diagnostic tests, they call, they call it the finger test or something, you know, the scalpel test where you just go on a plane where you think there might be. In, you know, necrotizing fasciitis and take a scalpel and get down to a fascial layer.
And if it doesn’t bleed but it produces, you know, a gray water, water like discharge, then that would be a confirmatory or a positive or increase your post-test probability. Um. Let’s be honest. I, I don’t think I would ever do that. Just they had
any sensation at all. Right?
Yeah. Right. And I mean, you’re, so we’re cutting into a known infected tissue.
Maybe, maybe if it’s really, you gotta convince a surgeon at bedside. Like, here, let’s go ahead and get that dishwater discharge outta here. Um. That would be, sure it’s an option, but you know, let’s be honest. It is, it’s unlikely to be the direction people go. I think we talk about it and I think I, it came to my mind as you described, the, uh, copious discharge that was coming from these wounds is very likely that same exact material that you find on a finger test.
So, yeah. Um, tell us again your antibiotic choice, because it sounds like you went right down the fairway. It was like a perfect selection.
Yeah. I mean, we did cef. I did Cefapime, vanco and then added Clindamycin, um, which I didn’t, you know. That was something that I, you know, obviously I ordered the CE Papine and the Vanko right off the, um, sepsis protocol, um, for the hospital.
And then, um, as I was talking to burn soft tissue, we were like, oh yeah, we need to add, uh, clindamycin. Um, which, you know, is, is I, as I remembered as I, through the whole process of thing for toxin suppression. Yeah. Um, can also be. Give a little bit of that better gram negative, uh, coverage. Um, you know, with Cefepime it has some, I’m not quite as good as probably some of our, uh, carbapenems, uh, but was, you know, kind of where I’d initially gone.
So,
yeah. That’s great though. I think that reminding, remembering the clinda for the toxin mediated suppression, that’s. Boards, like perfectly bo a board question. Um, I think Seines great, you know, you, who knows was what the risk of pseudomonas was, but, um, you know, traveling around Europe, having a walking boot on in now that’s totally f perfect or totally fine in that space.
And then at remembering the clinda, the clinda is the part that’s, uh, kind of gives us a little tip of the hat when we’re sending them to the OR or dealing with our consultants. So. Awesome, awesome. Um, and then the guy is like a textbook in some capacity outside of his paying out of proportion. ’cause uh, went to the OR and had to go back.
I was like, when is he, when are you gonna say that he is gotta go back? Because it’s always higher up and always harder to control. You expect it to be? Um, the CT is helpful. I think they were probably optimistic about trying to keep the knee, um, but repeat trips to the OR know that that’s gonna happen.
That’s, that’s not our wheelhouse, but, you know, that whole Steward Squadron know what you gotta know in one step further. Um, it’s an important piece to it, so,
yeah. Yeah. And the CT scan initially, you know, the, the air did track close to the tibial plateau, so that’s why they were trying to get it. And the margins were clear, um, on the.
Uh, on the surgical resection initially, but yeah, it just didn’t continue to be infected, unfortunately.
Yeah.
Yeah. That’s
how, how it goes unfortunately for individuals, uh, with this disease. But again, alive is alive, you know, above or below the knee alive is better than not. And so, uh, to that point, it’s not a, you know, it’s not an uncommon outcome.
To, to be dead to die from the process.
Yeah. Um,
I found, you know, as prep, uh, prepping for the podcast, the range in terms of mortality rate is all over the place. And a lot of that’s gonna depend on the time to presentation or the time really to the time to diagnosis. ’cause most of the time. That paying out of proportion drives someone to an emergency department a lot of the time.
Um, sure. So it’s misdiagnosis, it’s on our, it’s on us to catch it on that first visit, or ideally the second and not the third. Um, when it’s really progressed. So, you know, 20% all the way up to 80% mortality rate. I think if you’re gonna remember a number, probably in that 25 to 30% seems to be the most.
Typically cited, and again, is gonna vary by time to presentation or time for us to get the diagnosis correctly. Mm-hmm. Um, yeah, it’s a, it’s a scary disease. It’s a scary disease. Yeah, absolutely. Because what did we give in our podcast that like there’s no, like if I think this and I get this, I have the answer.
You know, there’s no specific element that can really put us there. Um, right. I never, whenever I lecture or even, you know, for podcasts like these talk about high index of suspicion, it’s a bogus term. We shouldn’t really use it anymore like we have to, obviously, I think you respect the disease knowing that you have something that’s got a 30% mortality rate, um, and has really hard to recognize, um, disease process and nothing that, and that’s
30% when treated.
Right.
Treatment for sure. Yeah. Um, so there. It’s something to respect and when you have something that’s hard and something that needs respect, that maybe raises your index of suspicion or makes you think about it more readily or should at least come up on your mind, you’re listening to podcasts like this and recognizing that pattern, you know, older diabetic, immunocompromised.
Pain out of proportion elements of the, of that scoring process with the low sodium, the creatinine problems, and the really high CRP, and then not just attributing to simple cellulitis if those feelers are getting out there, particularly with the really intense pain with cellulitis. So that’s a super awesome case.
So you, anything that you would do differently or what is your major takeaway on, on, uh, the care that you provided for that guy?
Yeah, I, you know.
As far as something to do differently, um, I probably would’ve given him some pain meds anyway back, even though he kind of, you know, uh, because anyway, yeah, that would be one thing that would, I would, I thought about later. Um, and you know, probably the other thing is just that, um. You know, it did throw me off at first, you know, just how dismissive he was.
Mm-hmm. Um, but I don’t think I’ll ever forget that in the future and will certainly just immediately unwrap someone’s foot. I mean, I talked to him, it wasn’t for very long, for a few minutes before I unwrap that foot. Um, but, you know, uh, it certainly has stuck in my mind as something. You know, as does pain out of proportion.
Right. When you first see that. The first time I saw a neck fa in the groin where they truly had, I mean, this patient acted like they had a kidney stone. Yeah. You know, and, and yet I couldn’t see anything on exam, but I was like, but this. They don’t look good. Yeah. And they have this pain out of proportion, you know, so that stuck in my mind, and I think this will stick in my mind.
Okay. So someone who’s dismissive like that, I can’t dismiss.
Yeah. Yeah. I have to
have, um, you know, to, to really do everything and see the patient, uh, for, for how they’re presenting and, uh, you know, rule outs, the worst things that it could be.
Yeah, I think that’s a great takeaway. Well, thanks so much, Shawn for joining us.
Uh, awesome case. Awesome disease process in its terrifying ness. I guess It’s awesomely terrifying and humbling. It’s a humbling disease process. Like I, you know, put in the camp of like aortic dissection where it’s just. Challenges, challenges. Challenges, and it was a cool one to go through. We’ll have some of the information related to the case, so you can do, you know, take a look at the score, try to get some of our, um, imagery there for you to review as well.
So take a look at the show notes at the bottom. And guys, thanks so much for listening and I’ll talk to you again soon.
All right. Thank you Jason.
Keeping your skills up in rare procedures is a constant battle. Time is not on your side and skills naturally decay. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off
Setting the Scene: Arrival and Initial Impressions
Triage Note:
Initial set of vitals: T: 36.6 °C (97.9 °F) HR: 100-110 BP: 96/51 RR: 16 SpO2: 95 %
“Pt ambulatory to triage c/o infected wound on right foot x 40 days, pt broke foot 40 days ago in Italy – was not given cast. Pt was unable to stay off foot and blister appeared – pt took amoxicillin with no relief. Pt tried to fix foot by putting a corn remover tab on the affected wound and it made it worse. Pt is clammy and warm during triage.”
Shawn describes a 40-ish male patient with a 40-day history of an infected right foot wound, initially described as a foot fracture in Italy. The patient presents with concerning symptoms like clammy skin and soft blood pressure, but no fever. The patient appeared unwell but downplayed his symptoms significantly.
Key Takeaways:
-Dismissive behavior from patients can mask the severity of their condition, necessitating thorough examination and not taking symptoms at face value.
-Unpacking the history is crucial, as initial presentations may not reveal the full extent of a patient’s ailment.
-We in Emergency Medicine are often as much detectives as we are providers. When a patient’s story doesn’t add up right, or the details seem off, dive deeper… this is often much more below the surface.
Physical Examination and Initial Diagnostics
A detailed physical exam revealed the man’s foot was in a bad way. There was malodorous and necrotic appearing skin, sloughing tissue, and probing to bone. The affected foot included blackened areas, dish water fluid discharge, and significant tissue damage, yet the patient reported minimal pain. Key vitals included an elevated heart rate and soft blood pressure, and lab results showed a high white cell count, elevated CRP and likely an acute kidney injury, though there were now priors for this patient. The differential diagnosis included an ischemic limb, osteomyelitis with associated soft tissues spread, abscess formation, and significant cellulitis. Shawn’s physical exam revealed the potential for crepitus- pointing towards severe infection, suspected to be necrotizing fasciitis.
Key Takeaway:
-A dismissive patient history or even a lack of pain can delay crucial medical intervention. La belle indifference is a term often used in psychiatric illness like conversion disorder, but a version can be seen in Nec Fasc (like this case), which may be from destruction of sensory nerves by the infectious process.
-Physical exam findings like odorous discharge and skin sloughing are significant indicators of severe infection.
-There is no one specific lab test for necrotizing fasciits, but there is a pattern to recognize that is captured in the LRINEC score, which itself does not have great test characteristics. Hyponatremia, markedly elevated CRP, and an AKI should be a pattern that raises alarm bells.
Patient labs- click to expand




Diagnosis and Treatment
Initial diagnostic imaging (X-ray) revealed gas in the soft tissues, leading to the diagnosis of necrotizing fasciitis. This was somewhat lucky. Not all Nec Fasc creates gas and gas may not be visible early- especially on X-ray. CT is more sensitive, but also can not be relied upon solely. Edema of the fascial planes outside of the area of skin changes is a key red flag in CT imaging.
The patient was started on a sepsis protocol with cefepime, vancomycin, and clindamycin before being transferred for surgical intervention. Despite advanced disease, the patient survived but required an above-knee amputation.
Key Takeaway:
-Diagnostic imaging and comprehensive lab tests can aid in identifying subtle signs indicative of severe infection.
-Minutes matter when dealing with necrotizing fasciitis. Once the diagnosis is made, sound the alarm bell and get the patient rapidly to an OR for wash out. Even with treatment, mortality is high… around 30%
Teaching Points and Reflections
The discussion emphasized the importance of considering necrotizing fasciitis in differential diagnosis despite atypical presentations (e.g., lack of pain). The use of scoring systems, imaging, and timely surgical consultation were key elements. Shawn underscores the takeaway to remain vigilant and thoroughly investigate when dealing with potential severe infections.
Key Takeaway:
-Early broad spectrum antibiotics and sepsis bundles can be lifesaving in severe infections, but is not the end point of care for the patient with Nec Fasc.
-Consultation with surgical specialists early is vital, as early surgical intervention can significantly impact patient mortality.
-In this case, the surgeons did not need convincing, but in cases without objective gas sometimes pain out of proportion is our canary in the coal mine. It can take some convincing of consultants not at bedside that you have a case of Nec Fasc. Stay true to you what you believe is going on to get the patient the care you think they need.
I personally like the line “I’d be happy to discuss why you think this patient does not have X (here Nec Fasc) at the bedside” 🙂
Conclusion
Nec Fasc most commonly affects middle-aged to older adults, particularly those with diabetes, peripheral vascular disease, obesity, or immunocompromise. However, up to 30% of cases occur in previously healthy individuals after trauma or surgery.
Necrotizing fasciitis comes in three flavors:
Type I (polymicrobial): older, diabetic, post-surgical patients.
Type II (Group A Strep ± Staph aureus): younger, healthier hosts, often after minor trauma.
Type III (Vibrio vulnificus): marine exposure, especially in those with liver disease.
⚡ Pain Out of Proportion is a classic early clue. It is severe, disproportionate pain compared to minimal visible skin findings — often described as “pain beyond what you’d expect for cellulitis.”
📊 The LRINEC score can help raise suspicion for necrotizing fasciitis, but it should never rule it out. Studies show poor sensitivity, meaning patients with low scores can still have NF. Always prioritize clinical judgment over the score. Knowing and identifying the abnormalities within the labs that raise suspicion for Nec Fasc can increase our clinical suspicion, regardless of the score.
🔍 The Diagnosis is Clinical. The most important diagnostic tool is bedside assessment. Rapid progression, severe pain, systemic toxicity, or skin necrosis should trigger immediate surgical consultation, even before imaging or lab results are available.
🩻 Imaging Can Support, but should not Delay: A CT with IV contrast is the preferred initial imaging when diagnosis is uncertain — findings like fascial thickening, gas, or fluid tracking along fascial planes support NF. However, if clinical suspicion is high, go straight to the OR, not the scanner.
Subscribe to the Podcast on



Podcast subscription form
"*" indicates required fields