Mastering Intubations: Learning Curves and the Quest for Competency
Contributor: Dr. Jason Hine
Understanding the learning curves in medical procedures is crucial, especially when it comes to such a critical skill as intubation. In this post, we delve into an Annals study of learning curves in intubation mastery. It sparks conversation about learning curves, forgetting curves, number vs competency-based medical education and, most importantly for us all, the maintenance of procedural skill.
Key Takeaway: The study emphasizes that greater experience in tracheal intubation is linked to improved procedural outcomes, specifically higher first-pass success rates and reduced hypoxemia.
Transcript
+
Hello everybody and welcome back to the SimKit podcast. I’m your host, Dr. Jason Hine, and today we’re gonna be talking about intubations. We talk about intubations and kind of learning curves, the gaining of a skill, skill maintenance, and a little bit about skill decay. Again, all of this will be focused around airway management and intubations, and is sparked by a paper.
It is Clark Brown Ward Etal Association between operator experience and procedural outcomes of tracheal intubation in the emergency department and ICU in the Annals of Emergency Medicine 2025. So what they did, this study conducted a secondary analysis of data from eight multicenter randomized trials of critically ill adults undergoing intubations in the US in emergency departments and intensive care units.
The investigators evaluated the association between the intubator or operators prior experience, number of intubations they performed, and key procedural outcomes. Of which there were two. One was successful intubation on the first attempt, which is legit, and two was the lowest oxygen saturation during the procedure.
Also, very legit. They use log log regression models, which.
Try to adjust for potential confounders such as BMI Apache two score the setting, you know, whether it’s the ED versus ICU and laryngoscopy type video versus direct. So the results, the sample size was 2,839 intubations. It’s a great number where they had known operator experience listed. The median previous number of intubations was 56.
Now, 65.6% were performed by critical care clinicians and 26% by emergency clinicians. You’ll notice that number doesn’t add up fully to 100%. There were a couple of anesthesia and other people in there doing intubations, but basically like a three to one ICU to Ed. So three times more done in the ICU.
Alright, so outcomes. The first pass success was lower than I would imagine, but kind of tracks with the literature, especially if we’re using, um, learners or novice intubators. It was 81.5%. How about SP O2? Overall, the median lowest SP O2 was 96%, which is pretty good. The key findings here was that greater operator experience correlated with higher first pass success and average SP O2.
We would expect this, right? The odds ratio was 1.75, which was statistically significant. But let’s pause now and take a look at the learning curves from the article.
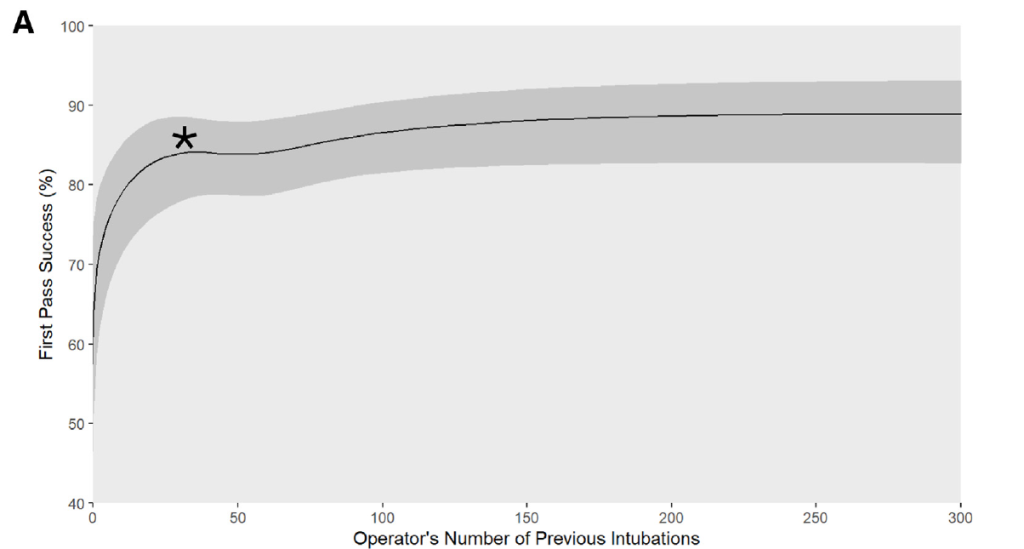
So here we’re gonna be looking at figure one, and we’re gonna start on part A, which was on the x axis, the operator’s number of previous intubations. And you can see here this tracks all the way out to 300. This is self-reported numbers, and we’ll get into that limitation in a moment, but that’s a huge quantity of intubations.
And on the Y axis we have that first pass success. Let’s really focus in on that zero to 100 scale. And as you can see here, when we start out around zero, you know, your first handful of intubations, your first pass, success rate’s probably around 60%, and it very rapidly climbs up to and above that 80% just spitballing here, maybe around 20 or so tubes.
And as we move our way toward 50, we see with this asterisk a little bit almost of an inflection point. Now the authors talk about a plateauing at 35 to 50, but we actually see that we are learning. There might be a slight regression as people get comfortable or confident, and then a very gradual and slight upward trend as we move through the a hundred, a hundred and fifty, two hundred, two fifty, all the way out to 300 intubations.
Interestingly, this same learning curve tracks throughout. So if we look at Ed versus ICU for Part B. The red is Ed higher than the ICU? I know, I know there’s probably reasons for that, but I’m happy to see that our percentages were higher. And then VL versus DL video laryngoscopy outperforming DL in section C.
So we see here that the learning curves show a very rapid upward swing, and I wish they almost shortened the X axis here for these figures, right? So we could see a little bit more clearly that first. Zero to 100 where most of the learnings happen, but we see a sharp upward learning. We see a bit of a plateauing or even a peak in a very slight downward trend as we move toward 50.
And the authors point out 35 to 50 seems to be kind of that sweet spot where people gain and maintain their skills. So. The authors note, the learning curves demonstrated that plateauing, as I said, in improvement after 35 to 50 intubations. Now, this is a really important concept and general number now in medicine and medical education and GME, we are trying to move more toward milestones and competencies rather than metrics or a number of times doing a procedure.
But these. Mile markers are important, especially in noting them in re in relation to our true learning curve. So that number, I’ll say it again. 35 to 50 intubations. We saw that plateauing of the learning curve. This suggests a threshold for procedural competence, which of course has to be tailored to the individual learner.
And we recognize that for one, you know, 35 to 15 to patients might not be the right number for all residents or all learners. But that’s a good mile marker or general sense for the average learner. We are gonna take that data and that number and apply it to the individual in front of us, the learner who we’re trying to teach, the skill of airway management.
But those are very important numbers to keep in mind on average. Alright. All right. Let’s talk about some strengths of the paper. It is a large multicenter data set across 16 US hospitals. This helps improve the generalizability. It is a prospective data collection with independent observers, which helps minimize recall bias.
We had some pretty good objective outcomes here, right? First pass success and oxygen saturation. These are relatively objective. Which helps remove some of that subjectivity here. And as we noted, the authors tried to remove all the confounders they could, and then the final strength of the paper, the learning curve analysis, provides actionable insights into training thresholds, which is pretty cool.
What about the limitations for the paper? The biggest by far is the self-reported experience, right. Operators may have over or underrepresented, or reported their prior intubations, and this makes sense. If you’re in this study and you just completed an intubation and it was smooth as silk, easy peasy. Oh yeah, sure.
When I’m gonna recollect on this, I’ve done it a hundred times, 200 times, 300 times as was reported with the learning curves. But if you had an airway, that was kind of hard. It was a challenging one to do. You’re more likely to underestimate or underreport your prior experience. That was tough. I struggled with that a little bit.
Yeah, I’ve done it 50 times. A hundred, 150. We’re gonna underreport how many times we’ve done it in the past. So people’s ability to recollect, or their recall is impacted by the success or the challenge and the intubation that they just did. And then there’s certainly the potential for residual other confounders, right?
As an example, experienced operators might have been assigned more complex cases, which is going to impact or bias the results, and these things are just hard to remove. They also had the exclusion of emergent cases, right? Patients that were too unstable for this study to be, for them to be included in the study.
For example, if they were in cardiac arrest or peri arrest. They were excluded, which again limits the external validity just a little bit. And then, you know, we also had limited, or it’s really hard to get data on the training method for the learners. It didn’t account for simulation based or didactic based training.
It really was based on reps, right? Number of intubations done. And of course, rare outcomes are hard to get power for. Right. The number of patients that are experiencing a cardiac arrest or progress to a, uh, surgical airway, they’re gonna be underpowered to find these elements. So that’s an important limitation to note as well.
All right, so the discussion, the findings here reinforce the concept that experience improves performance in critical airway management. We all kind of know that outcomes improved steadily for the operator and for the patient with a increasing experience until a plateau, even maybe a little bit of a tiny dip around 35 to 50 intubations.
These numbers are worth noting and being aware of 35 to 50 intubations. This actually aligns pretty darn well with the A-C-G-M-E procedural minimums for emergency medicine residents, which is actually 35 intubations. Now, the author suggests that the most skill acquisition occurs early within this range of 35 to 50, so this emphasizes the value of structured, mentored practice.
And the need for training approaches that can optimize competency during these early stages. And it’s worth now talking just a little bit about learning curves, but also for getting curves and skill maintenance. So let’s pull up a graphic to discuss. So the general process of learning and forgetting occurs like this.
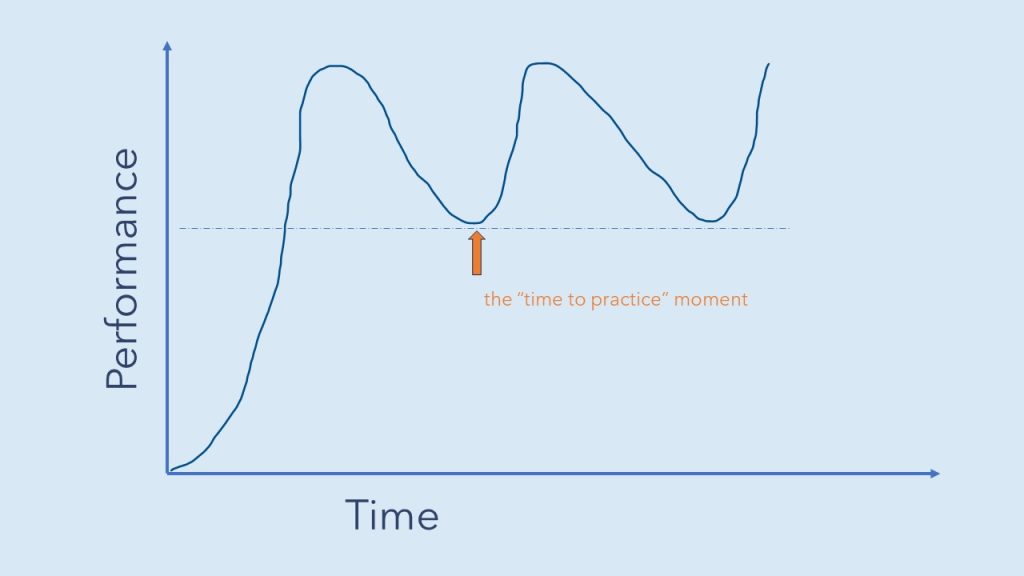
As we can see on our X axis, we have time, and on our Y axis we have performance. And if we compare this to the graphic from the the figure, from the paper, we see that over time there’s a very rapid, upward movement toward this dashed bar, which we have here, which represents competence or a person’s ability to perform this procedure independently without supervision, which is often the definition of competence.
So we move quickly up and above that competence level, and then we kind of reach a plateau as we saw. And for certain procedures, certainly procedures where we don’t get a lot of repetition in them, there’s actually the gradual movement away from confidence over time. And when we start to approach that dash line again, this is our time to practice moment.
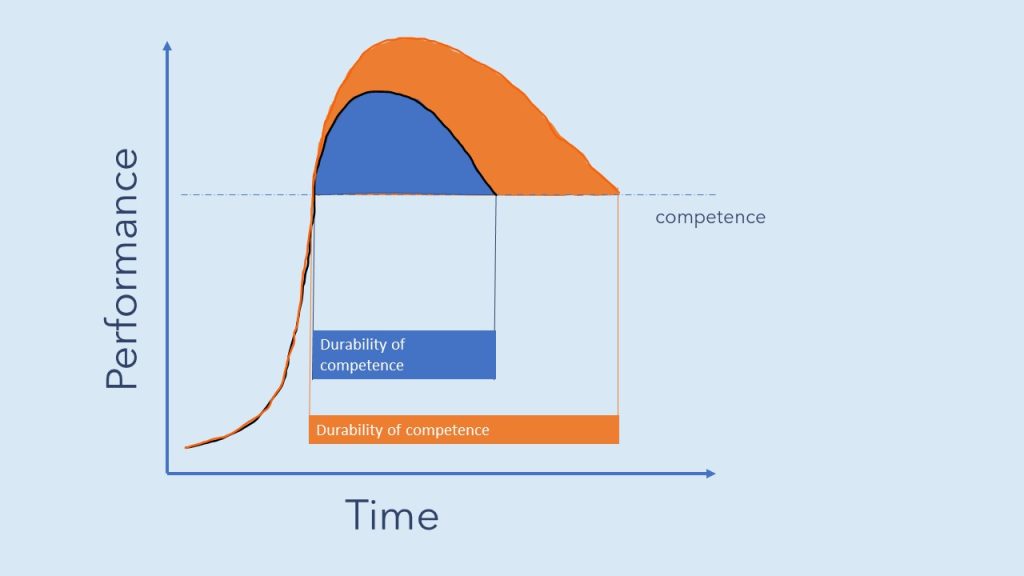
We retrain ourselves up, we get ourselves well above that line, it gradually drops back down, and we repeat the process of exposure over time. But interestingly, I think it’s worth talking about over learning a little bit here. So let’s compare the blue line that we just had with our orange line here, and you can see with the blue line ones, a learner gets up and above that level of competence.
They. Maintain it, and there’s a gradual movement back toward or down to that dash line of competence. And the area under that is what we call our quote unquote durability of competence, as you can see highlighted here. Now the orange line in our graphic is a person who, on an individual level worked really hard to not just get.
Competence, not just gain skill with the ability to successfully place a endotracheal tube through the vocal cords, but to do what’s called overlearning to learn and become tr a true master of the art of the procedure. They went well above that competency level and look what has happened to the durability of their competence compared to their colleague.
It has a longer period of time. Above that competency threshold and realistically, also the decay rate, the rate at which they lose their skill is also much lower or slower. So their durability of competence is much greater or longer depending on how you’re seeing it. So this is an important thing to think about and to train ourselves toward and consider training our trainees or our residents toward as well.
We don’t want them to just succeed at placing a breathing tube through the vocal cords, but we really do want them to overlearn to pursue excellence and mastery, and that’s going to improve the durability of their competence as they go out into clinical practice.
Okay, back.
All right, so an interesting look into learning curves, forgetting curves kind of space, repetition to main maintain skill, and this idea of durability of competence, which can be extended or grown by pursuing mastery or overlearning. Now let’s go over the author’s conclusions. They state that greater tracheal intubation experience.
Is associated with improved procedural outcomes, specifically higher first-pass success and reduced hypoxemia during emergent intubations in the ed. About a quarter to a third
fuck off. Delete that.
You are not helping.
Now let’s look at the author’s conclusions. They state that greater tracheal intubation experience is associated with improved procedural outcomes, specifically higher first pass success and reduced hypoxemia during emergency intubations in the ed, again, about a quarter to a third of them and in the ICU.
Competency appears to plateau after or approximately around 35 to 50 prior intubations. All right, well, what about our conclusions sim kit? We believe this is a robust multicenter analysis that substantiates the importance of experience volume in airway management training while the results support current procedural requirements.
They also highlight that competency is more than a numeric target. It involves supervised practice feedback and skill assessment. Future research should really integrate simulation-based learning, competency-based evaluations to complement this experience-based metric. Overlearning should be.
Overlearning should be reviewed on a more granular level to help understand the skill decay curve for airway management as well. But it’s an interesting concept to think about. Um.
Go back. Overlearning should be reviewed on a more granular level to help understand the skill decay curve for airway management. But it’s an interesting concept to think about is the idea of gaining or getting over the bar of competency that we should be training ourselves and our learners well above that bar so that they can maintain the skill for the long term.
Okay. Anyway, that’s all for today. Thank you so much for listening, and I’ll talk to you again soon. Let’s go back to that over learning idea
now. Now over learning should be reviewed on a more granular level to help understand the skill decay curve for airway management, but it’s definitely an interesting concept to think about is that rather than gaining or getting over this bar of competency. We should be training ourselves and our learners well above that so that they can maintain their skills for the long term.
Anyway, that’s it for today. Thank you so much for listening and talk to you again soon. I.
Keeping your skills up in rare procedures is a constant battle. Time is not on your side and skills naturally decay. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off
The Article
Association Between Operator Experience and Procedural Outcomes of Tracheal Intubation in the Emergency Department and ICU
Clark AT, Brown W, Ward MJ, Brainard JC, Brewer JM, Driver BE, Gaillard JP, Gandotra S, Ghamande S, Gibbs KW, Ginde AA, Hudson JW, Hughes CG, Janz DR, Joffe AM, Khan A, Lacy AJ, Latimer AJ, Mitchell SH, Page DB, Prekker ME, Rice TW, Russell DW, Self WH, Smith LM, Stempek SB, Vonderhaar DJ, Wang L, West JR, White HD, Whitson M, Semler MW, Casey JD. Association Between Operator Experience and Procedural Outcomes of Tracheal Intubation in the Emergency Department and ICU. Ann Emerg Med. 2025 Aug 22:S0196-0644(25)01060-1. doi: 10.1016/j.annemergmed.2025.07.008. Epub ahead of print. PMID: 40848028. [pubmed]
Overview of the Study
The study’s key focus areas were successful intubation on the first attempt and the lowest oxygen saturation during the procedure. The findings reveal that increased operator experience correlates with better success rates and oxygen saturation levels.
Key Takeaway: Experience is critical. With previous intubations recorded, the study found a significant improvement in procedural success with an odds ratio of 1.75, affirming the importance of practice.
Learning Curves in Intubation: The Details
Delving deeper into the learning process, the study showcases learning curves that highlight how experience impacts performance. The critical threshold appears to be between 35 to 50 intubations, where there is a noticeable plateau in skill acquisition (image 1). This aligns with procedural requirements, suggesting these benchmarks effectively represent competency.
Key Takeaway: While a numeric target of 35-50 is a useful guide, competency extends beyond numbers, involving structured, supervised practice and feedback.
The Importance of Experience: Getting Reps In
The sheer volume of experience plays a crucial role in mastering intubation. But don’t let that fool you, poor practice still equals poor performance. Quality practice is where it’s at.
The study’s large data set from 16 US hospitals enhances its generalizability, showing that critical care clinicians perform the majority of intubations (65%). Having high intubation volumes helps practitioners maintain high success rates and desirable outcomes even in challenging cases.
Key Takeaway: Experience and volume are essential in training medical professionals, with a consistent focus on skill retention and assessment.
Challenges and Limitations of the Study
No study is without its limitations. The main challenge in this one was self-reported experience, which might introduce inconsistencies. Additionally, complex cases and emergent scenarios were not fully accounted for, which potentially biases the results.
Key Takeaway: While informative, we have to consider the limitations self-reporting. As we look at the average numbers of intubations to gain “competence” (35-50) we should recognize the need for comprehensive evaluation methods in training, as there is not likely a “one number fits all”
Learning, Forgetting, and Relearning
For most things in medicine, repeat exposure is necessary for true retention, incorporation into clinical practice, and mastery. If we don’t use knowledge or skill, we do indeed lose it.
If you take the learning curves from the paper above (image 1) and plot out knowledge or procedural skill without spaced practice, it would look like the below graphic. With time performance wanes, and we have a “time to practice” moment. Hopefully that moment comes before a bad patient outcome.
Overlearning and Skill Retention
As individuals we need to think about overlearning—going beyond mere competence to achieve true mastery. This concept highlights the importance of continuous practice and skill enhancement, which ensure long-term competency and better patient outcomes (image 3)
Key Takeaway: Overlearning is critical for maintaining and extending competency. We should encourage students and attendings alike to aim for mastery rather than just meeting baseline requirements.
Conclusion
In summary, the article’s insights drive home the importance of experience, structured practice, and continuous learning in achieving and retaining competence in intubation and airway management. By understanding these learning curves, educators and practitioners can optimize their training approaches to produce skilled and prepared medical professionals.
By being aware of our own learning and forgetting curves, we can best prepare ourselves for long term skill maintenance by overlearning and engaging in spaced repetition.
Subscribe to the Podcast on



Podcast subscription form
"*" indicates required fields