Loud and Clear for the Room: improving communication in Emergency Care
Contributors: Ross Orpit MD, Will Berry PM, and Jason Hine MD
In this episode, we’re joined by Will Barry and Ross Orpit, co-hosts of the Loud and Clear Podcast, an EMS-focused continuing education platform built to bridge the gap between paramedic school and the realities of practice in the field. Will is a flight paramedic with 16 years of experience in EMS, and Ross is a board-certified emergency physician and EMS medical director with a background as a Denver Health paramedic. Together, they created the Loud and Clear Podcast — formerly known as EMS Cast — to give providers a set of guiding principles for navigating the uncertainty and complexity that classroom training alone can’t prepare you for. The conversation today centers on the intersection of emergency medicine and EMS: how we communicate, how we optimize handoffs, and how we can show up as the best possible partners for the crews bringing patients to our doors.”
Transcript
. Hello, hello. our Sim Kit listeners and welcome back to our podcast and our conversation today about emergency medicine and how we interact, how we communicate with our emergency medicine services, EMS space. So I have two guests to Doc talk with us today about this interaction, about how we can optimize ourselves, our environment, and a lot about a communication style hopefully is a direction we can go so that we can receive patients the best we can.
We can provide the best care that we can. So we’re joined today by Will Barry and Ross Orpi from the Loud and Clear Podcast. Will and Ross, tell the listeners a little bit about yourselves and the work that you do. Well, hey everyone. Uh, my name’s Will Berry. Currently I’m a flight paramedic in North Carolina.
I’ve been in EMS for 16 years. Started out as a EMT basic in the mountains of Colorado. Um, did most of my formative time as a paramedic in the city of Denver, which is where I met Ross, but I’ll let him talk about that. And, um, we’ve been doing the Loud and Clear Podcast for over six years now, and our goal is to, um, bridge the gap between that initial training you get as a paramedic and all of the hard knocks training you get on the street, um, as a, as a provider out there.
Yeah. Jason, thanks so much for having us. My name’s Ross Orbit. Um, as will alluded to, I met him working for the Denver Health Paramedic Division. Um, my path to EMS and medicine was very, uh, not straight lined. And when I finished, um, my undergrad, I thought I was gonna be a physical therapist. Was, was bored outta my mind in the physical therapy office and decided, uh, to go to medical school and decided to just get my EMT as some experience on my way to medical school.
Uh, I got my MT worked on the ambulance and fell in love with EMS, so much so that I put off going to medical school for. Four years and all in all, uh, in medical school and before worked for six years in EMS, uh, most recently at the Denver Health Paramedic Division. I did eventually go to medical school and, uh, finished and did my emergency medicine residency at Denver Health.
And then I did an additional year of training, uh, in EMS. So I’m a board certified EMS physician as well, and currently work in southwest Colorado where I work in an emergency department as an emergency physician, as well as provide EMS medical direction for some agencies in my region. Um, we, like Will said, I started the podcast, it originally it was called EMS Cast, uh, my fourth year of residency with another co-resident who was in EMS before going to, uh, medical school.
And we started it because when we finished paramedic school. There really wasn’t a lot of continuing education for paramedics out there. If you wanted to learn more after paramedic school, really all you were left with was physician podcasts or physician textbooks, um, which were fascinating, but a lot of it didn’t apply to you in the field, and that is why we created the podcasts six years ago.
Since then, there’s been an explosion of EMS specific continuing education, which is phenomenal. And so, um, will and I sat down and really got clear on what do we feel like people need now. In fact, we talked to a lot of paramedics to, to understand exactly what they felt like they were missing now after paramedic school.
And that led us to, to Reba rebranding the podcast, the Loud and Clear Podcast, um, because we wanted people to. Really understand what mattered to the patient in front of them. There’s a lot of high level nuanced discussions in education out there now, which is, which is phenomenal, but we can never lose sight of the forest through the trees.
And so that has kind of become our, our guiding principle. And in fact, our, our our, um, subtitle for the, uh, for the podcast name is EMS Guiding Principles, because at the end of the day, all this high level education is great, but we need a set of guiding principles so that we can navigate the uncertainty and connect that back to the patient in front of us.
And through that, and that, and that research has led us to create the paramedic confidence builder, um, which again, is all tailored to provide some specific coaching, mentorship, and foundations for newer paramedics to navigate this uncertainty and fill the gaps that were left behind from paramedic school.
Man, that’s fantastic work. And, and the audience can probably see how our paths have crossed because, you know, we we’re working in the space of skill decay. Maybe that’s a little further out. You’re certainly providing an unbelievable service to new paramedics and, and medics kind of looking and entering after, you know, the training and the safety net is in the rear view mirror.
So I’m glad we’ve gotten, uh, you know, kind of the kindred spirits together. Uh, thank you for what you’re doing in the EMS space, and so happy to have such experience and knowledge base on our podcast. So, looking forward to talking about the interaction, as I mentioned, I think the optimization really of how EMS and EM interact and work.
So if it’s all right with you, I’d like to kind of dive into this. I think of it in three categories or sections, preparedness, communication, and expectations. How’s that sound to you guys? Yeah, that sounds great. Let’s dive in. All right, let’s do it. So first one I want to get into is preparedness. So we talk a lot about this, as I mentioned in the sim kit podcast, about us as emergency medicine practitioners and how we prepare ourselves and really in a lot of ways maintain ourselves for the emergent patient, right?
There’s too many procedures out there that we need to be fresh on and smooth with skill maintenance, mental preparation team preparedness on a day-to-day level. What’s gonna come through your doors is really, uh, important to me and obviously something that, you know, we share in that space. So, so one interesting, um, thing, kind of like in the black box area for me. Is we receive so many of these critically ill patients, the patients that we need to intervene on rapidly halo procedures, all that space from our pre-hospital colleagues, but I have no understanding of their world of what they experience in that same area of skill maintenance, skill decay, those things.
So what is the process or structure out there? What recertifications might they be undergoing? How at risk for skillset decay are our paramedic colleagues? So long-winded way of asking you guys, tell us about this space and Ross in particular as you walk the line between emergency medicine and EMS. Talk to us about the contrasting or a similar landscape for the EMS provider and the EM provider, if you can.
Yeah, you, you know, it’s interesting when we, um, we did a little mini research project when preparing to create the paramedic confidence builder. And what we found is almost every paramedic, no matter their situation, whether they work in a big, busy urban department or rural department, experiences very similar challenges with regards to.
Getting better, preventing skill de decay and being prepared. And everybody faces it for different reasons. So if you work in a big, urban, busy department, your system is just so busy that despite having a lot of resources, you’re just trying to keep up with calls. So you don’t always have the time to sit down and train and dedicate some resources to helping train your providers.
Whereas if you work in a rural setting, you have the time, you just don’t have the resources or the manpower or the knowledge base to provide some of that training for your providers. So it’s a, it’s a real challenge, but it. It is the job of EMS is to be prepared for these disasters, to, to train for the unexpected, for the calls that you’re not always gonna see.
And, and the challenge becomes much more difficult compared to us in the emergency department where we may see, you know, 20, 30 patients every shift, they’re gonna see less than 10 every shift, and they’re gonna work, you know, maybe two to four shifts, uh, a week. And so the exposure becomes a lot less, and the opportunities for some of these things become a lot less, but the time sensitive nature of them doesn’t change at all.
And so the need to be prepared to still exist, and unfortunately, a lot of it has fallen on the onus of the individual paramedic to, um, decide how to maintain those skills. And that’s, that’s kind of what we created, why we created what we did, because that can be challenged if you don’t know where, what next step to take, you know?
Mm-hmm. Yeah, I would chime in, um, my perspective coming into this. So all of my experience prior to EMS was in the outdoor world. Uh, and that’s actually what got me involved in my initial emergency medicine exposure was guiding. And so something that I’ve reflected on quite a bit is in the outdoor recreation world, rock climbing, whitewater rafting specifically, there’s a lot of skills you need to have and your safety and the safety of other people depend upon them.
And there’s this, um, there’s kind of this shared tribal nature around it of like, Hey, if you’re not comfortable with that knot, like let’s practice it again. Like, ’cause if you don’t know it, well you’re gonna hurt me. You’re gonna hurt you like. Let’s just keep doing this. Tell, tell till it’s solid, you know?
Mm-hmm. And then going into paramedic school where that was an exposure for me of like, well, you only need to have five intubations on the books to get your certification. And so, and one or two of them can be on a mannequin if you don’t get the opportunity to intubate a real person. And for me, I was like, that just doesn’t feel like enough.
You know? I don’t, I know within me, I’m not comfortable with that because I just have, I’m self-aware enough of my skills to know, like I’m not good at it. Mm-hmm. And I think I brought that, that mentality for myself and of like, you know, if I am on a river and I tell the person next to me like, no, I’m good.
I got this. They’re gonna tell within about 10 minutes will don’t got this. And so. You know, that self-awareness. But, but within that, it’s a very loaded topic, right? Because people start to feel like an imposter. Like, oh man, I learned this. I should know it. Uh, is my friend gonna figure me out? Is my agency gonna figure me out?
I, I work with all these people that I respect, and I know, and they all seem to have it all together. And I don’t like, how, how are we gonna, how am I gonna pass this insurmountable, you know, hurdle? And so, you know, that’s something that Ross and I are really trying to overcome through the mechanism of community.
Mm-hmm. Of, Hey, let’s come together. Like, if you’re not comfortable with this, what can we do to help you get there? Because you’ve taken this huge step in self-awareness to say, Hey, I actually don’t feel like I’m, I know this very well. Well, cool. There should be people around you to say, like, let’s get you there.
Yeah. Fair. Some agencies do that better than others. Some agencies do have like procedure minimums for the year and if you don’t get, like say you know, your 10 intubations for the year, then you spend a day in the OR trying to get those intubations and that is phenomenal. But I know that there are a lot of agencies that that want to do that.
But unfortunately the ORs around them are also having to deal with, you know, a accommodate other learners. They’re having to accommodate, uh, you know, nurse anesthetists who are in school or paramedic students or, you know, and so it becomes challenging for them. And, you know, some ORs just aren’t willing to take learners or students.
So it can be challenging even if you want to do something like that. Um, but some people have like. Like, I’ve tried to implement in most of my agencies, like an annual procedure checklist to make sure that, uh, quarterly you have gone through these procedures with a trainer and somebody who has walked you through.
And I have, um, I’ve created a, like for the trainer, like, these are the things you’re looking for. These are the things you’re teaching on. And then for the trainee, uh, to go through, through those. But if you don’t have that, then it’s on your own. And I strongly encourage people to create their own checklists.
Like every quarter, I wanna make sure I hit these competencies and here’s my document for the things that, like, I’m gonna practice it and then look at the document and be like, what did I forget? I like that. I like that you’re in the space of kind of training the trainer. Um, and I, I recognize Will as well the.
The, we talk sometimes about known unknowns and unknown unknowns, right? And the most dangerous, I think is the unknown. Unknown. Who thinks that they are ready to hit, you know, hit their, their shift and take care of whatever comes through the door, come, you know, comes over the radio for you guys, uh, and doesn’t even recognize that they’ve lost their skill, that they’ve moved from competence to incompetence.
But then we get in this space and it seems like we’re kindred spirits again, of known unknowns. Okay. I know that I’m getting shaky on an IO insertion or an intubation or, you know, a lateral canmy for us. I. Can continue to fake it till I make it. I can keep that imposter syndrome going and just hope that it’s rare enough a thing that I don’t have to get called out by a colleague or have a patient with a bad outcome that puts me in an m and m.
Or I can lean into my community, I can lean into my colleagues and developing and refining and keeping these skills up. And it sounds like from a structural standpoint, it’s very site specific in EMS, just like it is in emergency medicine. It is. I, and I think to more directly answer your original question, I, I mean, I think, um, paramedic training, just, we just don’t get the same number of repetitions with some of these things.
And, um, it’s just the unfortunate reality. And that’s not knocking the accrediting bodies or, or the, um, certifying bodies. But like, we just don’t. And, um, our opportunity, you know, uh, endotracheal intubation is just the easiest skill to point towards. ’cause it becomes kind of a, it’s a critical skill. It’s time sensitive and it’s kind of a hot button topic in EMS, um.
Mm-hmm. But, uh, but we, our, our initial training requirement is relatively low. It is low. Um, the other thing is in this, there’s many tentacles that spread out the amount of research, the research we point to frequently has to do with in clinical environment instead of the pre-hospital environment. And then, you know, we.
We don’t know our frame of, sometimes we’re being taught by other paramedics that are in a similar boat. And so, you know, there’s, uh, some of this institutional knowledge is lacking, like some of that tribal knowledge isn’t always there. And so back to kind of what Ross said, some of the agencies do a really good job of owning this, taking it on and trying to fill these gaps.
And then some of them just can’t for either time, money, both. Mm-hmm. Um, so, and then, and then you get into this other piece too, of our, so many of the emergencies we lean into as paramedics on the street and physicians in the department is like, we’re not using any of these skills. This is like, you know, asymmetric problem solving.
Like, what are we trying to figure out here? Mm-hmm. Fair. Yeah. I think, uh, I, I appreciate that analogy and I. It sounds like there’s whispers almost of probably a higher degree of awareness and, and facing of a challenge. It, it’s always an uphill battle, right? Time, time doesn’t heal all in our space. It, you know, leads to skill decay and incompetence, but because of the breath and the, almost the austerity of the anticipation of austerity in that EMS space, maybe there is a little more recognition that just what you’re doing on runs is probably not adequate.
Let’s see what we’re doing in terms of our reps, the trainers, and the checklist, like Ross mentioned, is hopefully are maybe more robust than what I’ve heard from medical directors and departments who like, yeah, we have our, you know, annual CLABSI training and we have to do our central line, but outside of that, it’s just what comes through the door.
Um, so it’s an interesting shared experience for us, for sure.
Yeah, I, you know, I think in an ideal world, uh. Part of the job would be understood that, you know, you’re not just running calls and, and this is probably different for, there are busy departments, right? There are busy urban departments who are working not 24 hour shifts, but they’re working 10 hour shifts and they’re seeing 10, 12, 15 patients in that 10 hour shift.
And, and that like what training looks like for them is gonna need to be fundamentally different than the department that works like a 24 hour shift and sees maybe six, seven calls in those 24 hours. But I think in an ideal world for that department that is like more structured, like 24 hours, seeing six or seven calls, having an understanding that like part of the JO job is not just like running those calls and waiting for those calls to get it to come in, but part of the job is actually training.
So you show up and you train and sometimes that training gets interrupted by a call and then you come back and you go back to training. And that like having an understanding of like that is actually what your job is, is to be prepared. That’s awesome. That like gets me jazzed up ’cause that’s how we should all be thinking in that space.
And so yeah, thank you for kinda, you know, le letting us look behind the curtain a little bit, uh, in what it might be like there. And certainly gives, you know, if you’re a listener here, an opportunity to understand your local EMS, uh, operations. If you’re interested in education or even your own skill maintenance at all.
I’m gonna put a plug for reaching out and seeing if you can get involved in these type of training opportunities on a monthly, quarterly, whatever, even annual basis would be great for, uh, rapport, great for communication, team efficiency, and then your own skill upkeep. Um, all right, I’m gonna transition us a little bit.
I wanna, you know, we’re talking about our three areas and I wanna get a better sense of that communication. That was that second area. I wanted to pick your guys’ brains and so. As an EM physician. I know, I believe it was my intern year. I think it was like my second month. I did my EMS month rotation and I was in the back of an ambulance and I was nervous and a fly on the wall.
And then that was it. That was my EMS training in its own regard. Uh, you know, in terms of an experiential side, now during residency and after I’ve been involved in radio calls ad nauseum, we’ve all had more of those than we could count in terms of either listening in, asking our handful of questions, you know, something piques our interest and we come over to the, to the radio and see what’s actually going on there.
But I never really, through that experience, got a true sense of the training or structures that may be implemented by paramedics for arrival to the department. So, you know, Ross, and, well, I was wondering what education is out there for the EMTs and the paramedics. How adequate do you think it is and what supplements are you guys doing in the space of, you know, reporting?
I love the title of your podcast, loud and clear for the room, but like, how do we, what, what structures are out there? What’s part of paramedic training and then what is needed to maintain it thereafter? Yeah, first and foremost, regarding paramedic training, it’s very individual individualized, so, you know, um, just honing in specifically on the communication between the field provider and the hospital, for example, that happens different ways depending on where you work.
Some places you communicate with a phone, some with a radio, and, and so, and the expectations are different. Sometimes you’re expected to only call if the patient’s critical, otherwise you just show up. Sometimes you’re calling in a trauma activation based off that, that receiving facilities criteria. And so when you’re going through your initial paramedic training, you honestly don’t get a lot of training in this topic because they’ll say, they’ll punt it to your, your field internship experience because it’s so unique to where you’re gonna be.
And then. It’s on top of that, it’s gonna be unique to who’s training you. Right? And so are you getting good instruction or not? Like, you’ll, you’ll, some, some of it’s phenomenal, um, because it’s, that’s a, that’s a critical link between the field provider and the hospital. And some of it’s more like, well, if you say this, then you’re gonna get a big rise out of ’em, and that’s really what you’re after.
And it’s, well, that’s not, that’s not good, right? Ross and I are somewhat biased because we both worked at a phenomenal place that really Denver Health really cherishes the, the connection between the field provider and the the emergency department physician. Um, we would call on the phone and when we called on the phone from the field, we were gonna speak to a physician every single time.
We never talked to the charge nurse, for example. And so, um, there was a lot of pressure put on us during our training process of like, Hey, their time is important. They’re dropping everything they’re doing to give you their undivided attention. So you need to speak professionally, speak concisely, follow a format, and, and, you know, have this professional exchange with them.
Um, and so I think, and then that, that professionalism was reciprocated. So I think we, we really. We’re raised in a place that spoiled us in some ways, um, because it’s not like that everywhere. Mm-hmm. Um, some systems, you know, you make base contact for, for your A CLS algorithm, which is just, um, you know, seems like a waste of time to me.
Um, but, but yeah, it, it, it’s very dependent on where you are with that initial aspect of your training, and yet communication is such a pivotal piece of the patient’s journey and care journey. I mean, what’s this study that like, looked at, like 80% of medical errors can be tied back to like a miscommunication.
Mm-hmm. Um. I don’t know that around the country, like Will said, we were lucky to train in a place and we’re biased obviously by that. Uh, that took this very seriously. And, you know, in the Denver metro area, um, there was a physician at every handoff report. So when you showed up to transition care to the patient, there was a nurse physician, usually a tech as well.
So the entire care team was there. And that is important. It’s important to better outcomes for the patient. It’s important to more efficient. Care for the patient. It’s important to you as a physician. This is one of the things that I, I really want to get across, is how important this is to you as a physician.
It is not just an interruption in, uh, another interruption in your very busy day, but the paramedics have access to information that you will never have another opportunity to get access to. They know what the vehicle looked like. They know what bystanders set on scene who aren’t coming to the hospital.
They know what the house looked like. They may even looked in the fridge to see if there was any food in the fridge. Like there is a lot of nuanced information that will help expedite your care and speed the care of the patient in front of you and will also help you provide better care for that patient and help.
Prevent you from making a mistake or missing something. There’s actually a joint position statement and, and I don’t know the exact names of all the bodies on it, but it included like bodies from the nursing associations, the EMTs, paramedics, emergency physicians, and national EMS physicians wrote a joint statement saying that this is so important that the entire healthcare team should be present for the handoff.
Physician, nurse tech. The team who is caring for that patient should be there during EMS handoff. For that very reason. So I think it’s really important. I think that across the country, uh, I have heard unfortunately that is not the case, that a physician does not often show up for every handoff, and I think that’s a big miss and a big detriment to the patient when it comes to communication.
It’s also very different depending on what phase you’re in, right? So the communication and how you structure that communication and what needs to be communicated is different. If you’re doing the. Patient handoff versus if you’re doing a pre-hospital notification to let ’em know that you’re coming in.
Mm-hmm. Versus if you’re calling for online medical direction. And so if we take, say, for example, the patient handoff, right? We want to give a good, concise, comprehensive picture of, you know, what we saw when we were there, what we were told, what we did, and how things have changed since we’ve done those things over our time with the patients.
Um, when you, when you talk about the prehospital notification, we really just need to give the bare minimum information that is needed by the hospital in order to help set them up to be prepared for your arrival. And sometimes that’s like, this is a very routine, non critically ill patient. We just need a room sort of thing.
Mm-hmm. And there’s not a whole lot of information that needs to be communicated other than communicating that. Other times it’s like, uh, this is a sick patient and these are the things we need you to be ready for when we arrive. And then when we’re talking about online medical control. All of that is about creating a shared mental model.
Um, the physician cannot see what you see on scene right now. So you need to find a way to create a mental model in their mind over the phone to help them understand exactly what’s going on and the guidance you’re asking for, or the order that you’re asking for. Uh, so the, the online medical control is all about the mental model.
That makes a lot of sense. And it’s helpful to sort of think about the goal and objective of each of those different types of communication. And in my sim simplistic mind, I just thought of them all as communication, but there’s a lot of different motivators. And to paraphrase, and you correct me if I’m wrong in that space, the, there’s not a specific universal structure.
It’s not like, you know, Dubin, EKG, interpretation or every paramedic rate, rhythm access, interval hypertrophy, ischemia. It’s not that in terms of how reports are given in any of these areas. To Will’s point, a lot of that is gonna be. Location or geographically specific, which makes a lot of sense to me.
Doesn’t make sense to learn complex and, um, intricate presentation styles. When you go out and practice, everyone’s like, stop talking so much. We need just the base. You know, you’re gonna need to be site specific, region specific and case specific. Um, but so to confirm, there’s not necessarily a structure that is outlined that you have found in across your paramedics with whom you’ve worked.
Yeah. This is a really good point to clarify because just like in medicine and diseases, there’s not a clear structure for every single one of your patients that you see. And this is, goes back to what we’re doing. Podcast and what we focused our attention on is instead it’s a set of guiding principles for each phase of it.
So the, the principles are kind of what I just discussed. Yeah. Some structure is needed and, and we do teach some of the structure and we can get into some more of the detail of what the, like overall structure looks like. But especially when it comes to the handoff, there’s been some push for like some very tructure, uh, uh, structural handoffs.
So like, I missed, or sbar or some people are like very regimented to like, you have to follow this structure. And I push back against that a lot because I think the risk of of doing a very structured handoff is that the. Sometimes you forget to give information because you’re like, I can’t say that here.
I need to wait until this section. And then when you get to this section, you’re, you’re flustered by everything else you say you forgot to say that thing. So, so it lends itself to potentially leading you to, to actually forget information. It does help with remembering information too. So there’s a balance between the two.
Mm-hmm. The other thing it can do is it can cause you to bury the lead. So there may be a critical crux, uh, to this entire care, but it, it fits on step four of this handoff. Mm-hmm. Mm-hmm. So, so you don’t say it up front. And so as the physician or nurse is listening your handoff, they have a different mental model up until the point that you get to that crux and then everything in their mind suddenly has to shift.
Yeah. And so it also puts you at risk for bearing the lead. So I think structure is good, but having some flexibility within that structure is really important as well. That makes sense. And thank you for, yeah, that’s helpful to have a general sense. And we can put some of those, like, you know, we all know sbar, but some of those other, uh, structures that people might reference or utilize in the show notes.
Again, uh, encouraging a lot of cross communication after the podcast for our listeners for what their EMS crews prefer, what they’re taught, compare and contrast so that we’re all on the same page there. Um, I within this space, and Ross, I appreciated your direction there and even thinking about bearing leads, like you can get all the way through.
Patient’s, DNI. Okay. That really, that was the, that was the thing, you know, that we missed in the beginning because it wasn’t allowed until our structure, our very regimented structure, uh, allowed for it. But I, I wanna kind of get a sense about, and this is a very probably overly personal area to wonder about, is the balance of confidence and intrinsic doubt that comes with all of the medicine we do, but particularly for our EMS, uh, colleagues, which I think sometimes, you know, to use modern terms, it might be getting shade thrown at ’em from the e em crowd.
You know, we, in emergency medicine, we live and breathe it, but we still do to others. Uh, just everyone who’s provided care before you. There’s always that internal judgment that Monday morning quarterbacking, and as I said, you know, the cardiologist is gonna be, well, if you’re not really worried about a CS why are you ordering tropes?
Like, I, I can’t not order troponins in this, you know, 65-year-old with some chest funniness, even if he’s not describing it as pain, you know? So we know that that happens in medicine and we do it to our own friends and colleagues in the EMS space. We question, we critique, we monitoring morning quarterback.
And I suppose my question might be best asked in almost an example about being able to show confidence in the report, but doubt intrinsic to patient case. And so, you know, verbiage that might highlight that, which could further affect our degree of understanding or confidence in the EMS colleague is, you know, arrived on the PA to the patient and they were in vtech.
Is different than, you know, we got to the patient and they appeared to be in vtech. Or the one that’s super common for me sometimes is the initial pulse ox was 65 versus, you know, we didn’t have waveform or the fingers were cold. Initial pulse ox read as 65. And you see just subtle differences in portraying things that way.
And do you guys, you know, work in that space with your customers, with your, the people with whom you educate about maintaining confidence but able the ability to show some of that doubt that’s intrinsic in handoffs and the receipt of patients in busy field environments. Yeah, that’s, that’s tough. Um, I, I think underpinning all of this is if we all lean in with some healthy level of skepticism at all layers of the care, ultimately the patient should be getting better care, right?
Because maybe the next rung on the ladder sees something that I missed. Mm-hmm. Now, within that, what I would hope as a paramedic is to be treated with some level of respect. You know, like, Hey, let me tell you what I was up against on this call, and as you were, this is slightly a sidebar, so I, forgive, forgive me, but I, this call came to mind as you were talking.
Mm-hmm. Um, I was on scene of a standby for the SWAT team. And they were, they, they had a barricaded subject, so they had a bad guy in a house with an alleged hostage. Um, ultimately they got the bad guy out. They then swept the house and they found a woman in the attic hiding from him. So they get the woman out of the attic and they, she is not well.
Um. Mainly, you know, all they want her evaluated by paramedics. Okay. So I take care of her and, um, she physically fought with me nearly the whole ride to the hospital telling me things like, you don’t understand they’re watching. Mm-hmm. Um, they know that if once you go into the ambulance, you’re gonna, you’re gonna like rat them out.
Like, I don’t want to be doing this. But she, she needed to go for evaluation. She had sustained, you know, ungodly trauma at the hands of this person. They had just arrested. And when we arrived at the emergency, she kept saying, I’m gonna leave, I’m gonna leave, I’m gonna leave. And a lot of her, she could string together enough coherent thoughts to probably pass like a really quick capacity assessment.
So, mm-hmm. The, the hospital staff was doing their shift change. And normally, like Ross said, a physician would come to the bedside for the handoff and no one did. And I knew like if they. If they don’t hear my story and they just hear from her like, I don’t know why the paramedics brought me here. I wanna leave.
They’re gonna let her go. And she deserves an like, she deserves a workup. Yeah. And so I sought out the docs and thankfully one of them I knew and I just said, Hey, I’m really sorry. I know you guys are busy trying to do your pass off, but I really need to tell you about room 20 or whatever. Mm-hmm. And they were very appreciative of that.
And so I think where it relates back to what you’re talking about is A, being respectful and professional. Right. We all want to be treated that way at all rungs of the care. Mm-hmm. The other thing too is. As a paramedic, I need to recognize the limitations of my knowledge and skillset, but also be confident in the pieces that I have to give you.
That you have, like Ross said, you have no other way to get this information. This woman in my story, she’s not gonna offer up to the doctor. I was just held hostage in an attic for potentially days and like mm-hmm. Sexually assaulted. She’s not gonna tell anybody that. Um, and so like, my point is, it’s, it all of us have to check our ego a little bit, right?
Um, which is really d difficult to do, but, um, I need to arrive at your emergency department knowing I don’t know everything. Mm-hmm. But the things I do know, I need to make sure I’m confident in those things. I’m confident how I obtained that information. And then I can communicate that professionally to you.
I like that. I like that further highlighting of confidence of your experience. Right. And, uh, in that same space of balancing doubt and confidence, the things we’re certain of and, you know, have that obligation to the patient and the transition of care, you know, doubling down and maintaining oneself and having the, the sah to kind of, you know, do what you need to do, uh, as your example let along is, is valuable.
So I appreciate that. Hmm. Yeah, I think we often confuse confidence with arrogance or mm-hmm. Or we fear confidence coming across as arrogance and they are not the same thing. And one of the things I try to get across to paramedics that I teach is that one of the wisest things you can do is say, I don’t know that that doubt is okay.
That we live in doubt and uncertainty. This job is doubt and uncertainty. Um, and we just have to learn to navigate that and be okay with that and somehow still provide confident care through that. Um, there’s, there’s, when I was a paramedic, I often heard, you know, paramedic. As a paramedic, you are not always right, but never in doubt.
Um, and that can be taken well or that can be taken poorly. And that comes back to the confidence or arrogance piece of it is, is like you need to have the confidence in what you do know and what your principles are. So for example, the basics are always true. The ABCs are always true. You can always be confident in falling back on that even if you don’t know what’s going on.
And a lot of the rest of the case is in doubt. And it is okay to express that doubt. It’s okay to express that uncertainty. It’s okay for that to live because that is emergency medicine, especially in those first 10, 15 minutes. Mm-hmm. And so when you’re being asked about those things or when you’re being expressed about those things, you need to actually have the confidence.
To not know, to be in doubt, to have some uncertainty and be able to communicate that. And then you need to have the confidence to be questioned, to be asked about things, to have clarifications come your way to be able to provide those with like, here’s the things I’m confident about, here’s the things I’m not so confident about.
And that’s okay. Um, communication is a two-way street though, right? As well. So us as emergency physicians, one of the most important things we can do is not interrupt. One of the most important things we can do is, as they’re giving that handoff, as they’re giving the report, is to stand there quietly, and listen.
Don’t try to multitask, don’t try to do a physical exam while you’re doing it. We cannot multitask. All we can do is task switch, which means we’re switching off of listening to the, the information they’re giving us. And so, stand there, take in the information and hold your questions until the end. Then when you do have questions, ask them respectfully and professionally.
And so, you know, you may say something like, okay, so when you arrived, you mentioned the pulse ox was 65%. Did you, did you happen to see the waveform with that? Like, are you con was a really good waveform, are you really confident that it, it was 65%? Um, and all you’re doing is clarifying, like I’m just trying to get a clear picture, like yes, we are confident it was 65% or maybe was there some a, some ambi ambiguity there?
’cause right now it looks different, but maybe it’s different because of the things you did. Mm-hmm. And so I’m just trying to make sure here. Um, and then the other thing I always say is like, you know, best practice is usually to praise in public and reprimand in private. Mm-hmm. And so if you do have some constructive feedback, unless you have a great relationship with that, where you can like.
Some of my, some of my paramedics have pushed back against this because they were like, no, people need to see that this is okay. Like people need to see that, like constructive feedback is okay and it’s, it’s good for me to get it and learn and receive it. Um, but others not so much. Right? And so, like, unless you have a really good relationship with them, sometimes it’s best to like pull them aside, go out to the ambulance bay, and then have a, like a private discussion about like, Hey, here’s, here’s what I noticed.
Here’s maybe what I think could be better. And, and honestly, as a paramedic, you should eat that up. And as a physician you should make efforts to do that because everybody wants to get better and everybody wants to understand how the other works and what the other is looking for and how we can work best as a team.
And so I think that’s best practice. And if we’re all confident enough in ourselves, we’ll be able to have those conversa conversations openly. Yeah. I, I want to add another thing too. You know, so much, so much of what a paramedic wants is they want to feel like, you see how, how much of a challenge they just went through.
Mm-hmm. And so our skillset is narrower and it’s, it’s very defined right. At, um, those initial moments of a critical patient. And so within our small piece of medicine we’re doing, we’re making some of the same critical decisions that you guys are in the emergency department, just but within our small window.
Right. And all we want to hear sometimes when we get to the hospital is, good job. I would’ve done the exact same thing. Mm-hmm. Or, I’m seeing this a different way. Lemme tell you what I’m seeing and have a professional back and forth so that when I see it next time, remember a lot of times paramedics are out there alone.
Yes, they have a partner, but in some services a paramedic is paired with an EMT basic, which means they’re the only person on that scene with their level of training. And so they’re trying really hard to do the right thing with their limited tools, experience and training. And so to have the physician in the emergency department say, Hey, good job.
Or, Hey, I’m, I see this slightly different. Let me point out to you what’s informing my decision about my care. You’re like, oh man. Awesome. I can take that with me on my next interaction. If you truly understand and and convey, you know, that, that in the pre-hospital setting, outside of your four sterile walls, like things are chaotic and incomplete and constantly moving and abbreviated, like Will mentioned, it can help if you have some grace for the somewhat lack of information that you wish you may have had.
If you’re able to express that to the provider, they will likely give you more leeway with the clarifying questions you have for them. I like, I mean, there’s so much, so much awesomeness in what you guys just said. I’m gonna try to do a quick summary. I think one, a awareness, you know, it’s easy, as I said, for a cardiologist to question our orders.
It’s easy for us to ask like, why didn’t you do this? When we have absolutely no understanding of the scene, the person, you know, in the rig with them, uh, the fact that they might be operating alone. All of those elements that we just. Assume they have a similar structure, similar support system that we have.
I really like the, you know, uh, I’m gonna, I’m gonna botch it, I think Ross, but the praise in public and, um, you know, critique in private, uh, that general sentiment and even, I know I’m at fault in this regard. Just the simple, like, awesome job, man, that was a fantastic report before carrying on with a patient probably builds relationships more than a lot of the other things that we think that we’re doing.
Um, and so those simple little elements there, and as you guys were talking in this space, I think it comes down to just simply humanism, uh, pro being overly philosophical and waxing here, but, you know, I’m a spouse, I’m a father, I’m a son, and just the way we communicate with one another in these ways is no different than how we talk to our.
Significant other, for an example, you know, the i versus the you statements and like the, how confident were you in that waveform or, you know, um, those types of questions versus were, you know, were you confident in or how confident those, the way you phrase those parts, um, are really important. And, and just being sort of thoughtful and uh, trying to avoid anything that could be seen as a insult or a critique on the quality of care that the person is, uh, is giving I think is important.
So, you know, what’s your degree of confidence in, I actually was stumbling over this as I was thinking about it. What’s your degree of confidence in that waveform is probably better than even. How confident are you in that waveform? So just thinking simply about how we ask those questions and the insinuations that could come with them, I think can go a long way.
Yeah, absolutely. All right, I’m gonna carry us forward. I feel like I could continue in that space, but I appreciate all of that, uh, information in the communication space and also getting into what is, you know, notably a touchy subject, but one that I think if we don’t think about it becomes more touchy in real time when we’re trying to get some information about the natural doubt that’s intrinsic to medicine versus doubting the, you know, provision of care beforehand.
But now I wanna ask a little bit about expectations and, you know, as the receiving institution, as a receiving clinician, what is allowable, I guess, right? So request expectations for EMS personnel via, via, uh, the radio or, you know, anything really prior to arrival. We talked about it being, uh, on telephone in different capacities.
And so if it’s two sided, I think, you know, there’s the element of what can we as the, uh, command phone holder or the EMS person receiving the patient, what can we ask of our paramedic colleagues prior to arrival? And then sometimes, um, particularly I feel like in the critically ill or pediatrics, I want that patient brought very rapidly to my er.
And the asking of stopping or not doing things that are within the scope of practice of the paramedic, that is also a bit of a touchy subject. Right? So to explain this, again, more by examples, right? So in a person that we want to rapidly transport, asking or saying, you know, please don’t. Progress to intubation in the field.
If you’re comfortable doing so, place an LLMA and transport expeditiously. I think that sounds good to me, but I don’t know from your guys’ perspective. So what recommendations can you give us, EM, providers about those two sides? Let’s start with the. What is a reasonable request in the stabilization or, um, work done by our, uh, EMS personnel.
And then we’ll hit the Please don’t do that side after sound. Okay. Yeah. Yeah. I think, you know, some of this comes down to having an understanding about, you know, what they can and cannot do and the limitations of, uh, the scene, the limitations of their ambulance, the limitations of their equipment. And so this is a shameless plug to learn more about your EMS systems and what equipment they have, what medications they have, what is within their scope of practice for their level of certification.
And one of the best ways to do that is just if you don’t know, like, if you ever have that thought of like, I wonder if they have this medication. I wonder if they can do, just ask. You know, sometimes as physicians we’re a little embarrassed to ask too, ’cause we feel like we’re the ones who should know.
Right? Um, but the more you ask, the more you’ll learn and the better you can work together and as a team. So I think that’s, that’s the first principle. The, the second thing I would say is this again gets split up by where we are in the phase of, of communication. So if we’re talking about when it comes to the receiving the pre-arrival notification mm-hmm.
Remember that in that moment you do not need all of the information. The time will come when the patient’s in the emergency department where you can ask more questions. And the questions you need answered right now is purely what will change your response and preparation prior to their arrival. Mm-hmm.
What information do you need to know to make sure that you are ready for what is about to walk through the door? It needs to be brief. You need to keep it brief. ’cause they have more work to do on the way to the hospital. They’re coming with a sick patient and they have probably about 10 things they want to get done before they get there.
One of which is to let you know, to be prepared and so. If the patient is sick and they have more work to do to continue to care for the patient before they arrive, try to keep it brief and just get the information, you know, and I have actually a bio phone call, uh, that I’d like to play that kind of highlights this principle pretty clearly if I can.
Absolutely.
Did you base Dr. Sanko? Go ahead. Oh yeah, Garcia on three, four game. Me. Okay. Yeah. Hey, we’re code 10 you with a thirties male self fl stab wounds. Um, had some pretty deep lacerations to the bilateral arms and probably about a man like a foot long, uh, laceration. Kind of from the left shoulder to the left.
Abdomen, it looks like adipose tissue but no lungs affect. The blood pressure right now is 60 over PAL, and we’re probably about five out 60 over Palp. Yep. What’s his pulse? 120. How much blood was there on the scene? Oh man. I’ll talk to you when I get there. Probably about two liters. Okay.
So this is a perfect example of like what information did, do you need to be prepared for that patient. You need to know what the mechanism wa of the injury was. He was stabbed. You need to know where the stab wounds were because you need to know what you need to be prepared for. So you know that he has extremity stab wounds, so you may need to tourniquet.
He has stab wounds to the chest and abdomen, so you may need to be prepared to place a chest tube and you know that he’s hypotensive, so you’re gonna need blood ready. Like do you need other information than that to be prepared for this patient? You may want what the pulse rate was. You may want how much blood there was on scene, but if we’re honest with ourselves, that is all the information we need to be ready for that patient.
So keep that in mind. Understand that he’s flustered in the back of the ambulance, trying to get two lines for you, uh, and, and do everything that he needs to do before he arrives in the hospital. And to, to tag, tag onto that. I, I think when you hear that initial ending where you’re like, oh man, I’ll tell you when I get there.
I’m sure most physicians are like, how rude that paramedic might literally have his phone under his ear like this while both hands are trying to control a hemorrhage. And so I’ve been in very similar situations and you’re, you’re, you’re not an octopus. You just don’t have eight arms. Yeah, no, I, I appreciate those elements and, um, the, again, leading with the, not bearing the lead, that blood pressure early on, obviously super would be nice to have early in that report.
And then the practitioner, the EM provider receiving like areas involved know the, know the blood pre, you know, know the degree of extremist the patient’s in, let me go get ready and let you do what you need to do. Yeah, exactly. And so then when we shift to kind of more what maybe your question was tailored towards, is that online medical control?
Like I’m calling for this order or for guidance? I think I really like what Will talks about, uh, when we teach our paramedics with regards to this, when they may be frustrated about not getting the answer they want. Or sometimes the physician is like, you know what, just don’t do anything. Bring ’em to me.
Uh, and, and I’ll figure it out when they get here. So I, I’ll turn it over to you Will to talk about that a little the first thing you need to do when you, when you get a, when I, as a paramedic get a response from the physician on the phone that I’m unhappy with, the first thing I need to do is think about what did I just, I need to reflect what did I just do to, to, to not paint the best picture of the care I’m providing.
The, the other thing that I need to reflect upon is if I’m getting an answer of like, oh, man, just bring him here. Then I obviously didn’t paint the picture to you of what I’m seeing and, and accessing. And then I also am not asking you for anything specific. Um, if I, if I, um, just sound chaotic and flustered and like, I don’t have my care together, and then I’m putting you as the physician on the other end in a, in a spot of like, now tell me what to do.
Of course you’re gonna say, gee, I don’t know. Why don’t you just bring ’em here so I can see them with my own eyes? Mm-hmm. Because I can’t tell you what to do. And so the big thing that we try to teach people is when you call and ask for something, know what you’re asking for now, also be open to suggestions and ideas and, oh, I didn’t think about it that way, or whatever, but lead off with, you know, Hey doc, I’m calling for an order for an amiodarone drip.
And then go into the story to paint the picture. Well, all of that. And then at the end, Hey Doc, what do you think about that order for 150 milligrams of Amio over 10 minutes? Yeah, so this goes back to that principle that the point of this phone call of this communication is creating that shared mental model so that we can be on the same page of what is going on with the patient despite being in two different locations and come up with a consensus of what is the next step forward for that patient.
So being clear with your ask, like Will said, one of the most important things you can do from the paramedic side is state upfront why you’re calling. Because as a busy emergency department physician, we are constantly interrupt. We’re interrupted what? Like every 17 seconds I think the study showed. And so we’re constantly trying to task switch between a whole bunch of different things.
And so when you call us with something, you need to make sure that we are in the right mental space. To hear what we need to hear to help you out. So whether that’s, Hey, I’m calling for this med order. Great. I know the medication, I know what indications that medication is used for. So now I know what I need to hear to be confident to give you that order.
Or I’m calling for refusal. Okay? I, I know what I need to hear to know that they have capacity and that it’s not a super high risk refusal. And I can give you the okay for that. Or sometimes you need to just be like, Hey, I got a weird one and I don’t know. I need your help. And that tells me, okay, I need to really stop anything I’m doing right now.
Sit down and listen closely. ’cause this is, this is gonna be odd and I’m gonna need my full mental capacity to help you navigate this situation. And so teaching your paramedics to do that for you so that you can be in the right mental space to answer the questions they need and develop that shared mental model.
Um, I have another example here that highlights trying to get to that shared mental model with the paramedic on the other end of the call so that we can get to the right answer for the patient hey, this is paramedic McFarland, DGA 37. You hear me? Okay? Yep. Go ahead. Calling for a field pronouncement with what appears to be a DNR in place. The advance, but it’s like a, it’s not like a state DNR. Sure, sure. Appears to be a living will. Sure. It says under terminal condition, it says, I direct that life sustained procedure shall be withdrawn.
Order fill pursuant to the terms of this declaration, it being understood that life sustaining procedures shall not include any medical procedure or intervention considered necessary by the attending physician to provide comfort or alleviate pain. We got signed by her, signed at the end by a physician and her and two witnesses and a notary.
Mm-hmm. You good with that? Yeah. No, just so what, so gimme some story. But I, I mean, probably she’s in, but yeah, she’s in cardiac arrest. How old? 81. 81. Okay. And is there like a terminal illness or like, do we know a mass past medical history or, uh, no. She’s got a history of hypertension, was found down by her husband.
Husband tried to start CPR by husbands living wound place. Okay. And is the husband okay with that? Like, how does the husband feel about this? Because, you know, this is, so, this is, I mean, granted, I appreciate that like, you know, she’s got all this documentation, but like you said, this is not like the state most form, you know?
So, you know, like how does the husband, what’s the husband doing? Uh, uh, I’ll, I’ll talk to him. So we can, we can stop it. There will, but that is an example of like, there is a complete disconnect. That physician who cannot see what you can see, who does not understand everything that has led up to that point, needs to somehow find a way to navigate developing that shared mental model with you.
Mm-hmm. And so you’re on the paramedic side of the call, like your, your job is to try to create that shared mental model. If you’re a physician, your job is to try to get that shared mental model and to do it professionally and find a way to tease that out so you end up on the same page. Um, I’ll pause for thoughts there.
Yeah. No, I, I appreciate these sort of thoughts and consortium, and particularly those, uh, examples, and you can see in that second one where the physician is going. But I think, again, lacking awareness of on scene, provision of care. I don’t know if they’re actively coding this person until they’re given permission to stop.
Oh, there’s a lack of awareness. Like it sounds like this is in the setting of a potential terminal illness. We’re fair to proceed forward so long as this is a shared opinion by. Those involved that can verbalize themselves. So can we confirm with the husband that this document should be adhered to right now?
That little bit of information to explain that mental model would go really far for this. Guy’s like, okay, now I gotta go talk to the husband. I’ll be back. Like, that’s not a great communication, uh, at the end of that, that, that audio clip be played for us. Yeah. And as the paramedic, I think about too, like there may be some, if there, if, if this is bubbling up to calling, um, there may be some bizarre social setting mm-hmm.
That it’s on that paramedic to, to tell you about. Um, and I, you know. For example, people threatening you like, start CPR or I’m going to, I’m gonna shoot you, or something like that. Mm-hmm. Okay. You know, like, I need to make sure you understand all of the situations that I’m up against so that we can make the dec the shared decision in the best interest of the patient and in, in best interest of safety for everybody.
Yeah. So this sets us up with, before we can give any recommendation whether we give approval for the order or we, uh, request that they do something different than what they originally wanted to do. Before we can do any of that, we need to have this shared mental model. So that’s why that is the guiding principle of this phase of communication.
Now. If we get back to your question about like how do you handle saying, actually I want you to do something different. Mm-hmm. It’s in principle, we need to somehow convey our mental model of why we want to do something different with the paramedic. And so once we have a shared mental model, what’s going on, we may have a different opinion because of whatever knowledge we have, maybe whatever education we have that is telling us maybe we should do something different.
We need to find a way to concisely and professionally then relay that to the EMS clinician on the other end of the phone call, like, I hear this, this is my understanding of the case. This is my understanding of what you want to do. I think it would actually be best to do this other thing, and here’s why.
Here’s where my mental model is at. So I have another call that kind of highlights, uh, this. So in this, uh, call, the paramedic actually did a phenomenal job of creating a mental model of exactly what was going on at the time, um, but wanted to do one thing and I actually recommended he do something else and tried to explain my mental model as to why hey there, paramedic Lee on DG 16. Can you hear me okay? I’m rhythm checking 30 seconds loud and clear. Hi, I’m calling for pronouncement. Uh, I’m met with a 52-year-old male, uh, sudden cardiac arrest in front of witness stop, or was witnessed with, um. Not so great bystander CPR when we arrived. He was an asystole.
We’ve been working him since 1321. He’s received three milligrams of epinephrine, uh, and two milligrams of Narcan. He was aole epi until about three minutes ago. We have an organized PEA at a hundred, uh, solid 7.02 with a tidal of 50 at this time. Um, still pulseless with that PEA rhythm at a hundred. Um, unknown etiology.
He does have an inhaler on him, but other than that we don’t have any history. He’s got a hematoma to the forehead, um, from when he fell per bystanders. Um, do you have any questions for me? So you have a, a 52-year-old gentleman who was a witness. Cardiac arrest received bystander. CPR was initially asystolic, but now has an organized rhythm at a rate of a hundred and has an intital CO2 of 50.
Correct. It seems like you guys should probably continue a CLS efforts, uh, and consider transport to the hospital. Just given he’s got a lot of positive, uh, factors going in his way. It was witnessed he got bystander CPR, it’s been less than 30 minutes and you’ve had a improvement in his rhythm from a CLS or from asystole to PEA.
Organized at a hundred and he’s got in title That’s good at 50. Alright. We will transport. Do you wanna give, uh, Rosa a heads up? Probably 10 minutes. I’ll give Rosa a heads up. Thanks. Thank you.
So you can see there as I was, I was hearing all that and I could, I could see your face, Jason, as you’re taking all that information in as well. Your head kind of starts to turn and you’re like, there’s a lot of positive predictors of this patient could have a good outcome. Mm-hmm. And so now my job is to somehow get the paramedic onto that mental model with me, uh, to maybe take this call in a different direction.
And that patient may have had Rosc and is just profoundly hypotensive, right? Yeah. At that point, right. They might just be non palpable and you throw a probe on and you see pulsation pulsitile movement. I like it. And so I like the mental model idea. Sorry, go ahead. Will. No, even disrupting that paramedics, uh, and when I say disrupt is maybe a word that we conjure up confrontation, but I mean, like that paramedic has been in this mindset of like, we’re working this a systolic arrest that seems like it’s gonna have a poor outcome.
And, and breaking their cognitive bias a little bit of like, Hey, you may have actually achieved Rosc. Um, you, you know, you would hope that a, a mindful, um, you know, truth seeking medical would be like, oh my gosh, you’re right. Uh, yes. Thank you. Like, I need to switch gears. Mm, mm-hmm. I like that. And, and, uh, Ross in, I don’t know if there was a shift change or if you’re able to do so, but uh.
Without getting too much details of that case. Um, do you know, like, uh, would you offer or did you do in that situation, the sort of away from others, uh, debrief with that person? Did you talk about the options? I mean, you did such a concise and good job of explaining your mental model on the radio that it might not have been necessary, but how would you recommend rounding out that communication with that medic after the fact?
Yeah, definitely. Um, I think if you have the opportunity, you should take every opportunity to do that, um, because it’s going to strengthen your relationship with that medic. Uh, it’s going to strengthen their trust in you when you’re giving them advice over the phone. Um, so yeah, so this is a big busy system and I didn’t see them for the rest of the day, but I did have the opportunity to go to the division afterwards, discuss the call with the, uh, supervisors as well as that paramedic and just have a debrief afterwards to be like, Hey.
Do you understand where I was coming from? Like we, we only had a limited time on that phone call, but I just wanna make sure like we’re clear. Uh, you understand where I was coming from? I’m, I’m not trying to make your life harder. Mm-hmm. Um, and so and so, yeah. And they were very understanding of that. I, to your point, actually had a recent, um, call that did.
I did not. I I gave you one where I looked very good. Uh, I had a recent one where I did not do so well. And this was, this was fairly recent and I reflected on it and I actually pulled the, the paramedic aside. So he called me with a kiddo who had, uh, was having seizures, uh, and he had given benzos. It was like a, a 5-year-old, no history of seizures, has given benzos, was still seizing in front of me, uh, and asked me what to do.
And I said, what are your vitals? Uh, and he said, I don’t have any right now. And I said, do they have a pulse? Uh, and he is like, yes. And then I was like, okay, I’ll wait for a blood pressure and. Reflecting on that case, this going back to like, what do they need in that moment? Mm-hmm. What do they need from me and what do I need to know?
They don’t need me to harp on the importance of vital signs. Like what I need to know in that moment to help them out is to A, understand that they have a five-year-old in front of them and turns out they have a five-year-old at home, um, that they’re, this is a high anxiety provoking call for them.
Mm-hmm. They have given the normal algorithmic type response and they’re, it’s not responding like they would expect it to. And so they’ve hit the end of their algorithm and they ne now need help navigating that further. And what do I need to understand? What do I need to know to help them navigate that?
What I need to know is that they’re managing their airway and that they have a pulse. Mm-hmm. And they manage the airway and they have a pulse. We can move forward and I can talk ’em through like, yes. Is having a blood pressure important? Yes. Do I need it in that moment to help them move forward? I do not.
And so what I wish I would’ve done in that moment is assured that they were managing the airway, assured there was a pulse, and then told them to give more benzodiazepines ’cause they don’t have access to other medications. And then I would’ve said, please work on a blood pressure and access on your way.
We’ll see you when you get here. We’ll be ready. Um. So that did not go well. I did not do well on that call. And after the fact, uh, because they brought him into my emergency department, I was able to pull that paramedic aside afterwards and apologize and say, Hey, I, I was poor on that phone call. That is not what you needed from me and here’s what I wish I would’ve done instead.
Um, and we talked about, you know, we did some education surrounding the call and what was going on, and, and he shared that he has a, a little one at home. So that was producing a lot of anxiety as well. And so, so you’re absolutely right that that ability to debrief after something like that, uh, can go a long way for these.
There’s one more scenario that we don’t have an example of that I do teach paramedics about that I think is valuable to discuss with physicians and that that’s utilizing you guys as a tool. Mm-hmm. Um, now we’re, we’re kind of doing that all of the time, but I wish we had the recording. But one of the very few times when Ross was in his physician training, and I was still in the field that we talked to each other on the phone, um, was a, basically a high risk refusal, um, out at the Denver International Airport.
And so this, this gentleman had experienced chest pain on his flight. Um, they had asked for paramedics to meet them at the gate. Um, he had some, he was not having a stemi, but he w he had some, uh, I think T-Wave inversion, something, you know, on his EKG that we have. We have one EKG. We have no way to know if this is normal for him.
Um, he is adamant I don’t want to go to the hospital. Denver was a stop along the way. He was trying to catch a connection flight and his family was even worried about him and he was like, no, we’re going to wherever, Cancun or whatever they were going to, we went so far as to as to tell him, you know, sir, you could be having a heart attack, or this could be the start of your heart attack and you could get on your next flight and you could die.
We told, we went up to saying he could die, and he said, no. And I, we have one tool left in the toolbox at that point, and that is to call it the doctor. And, you know, paramedics need to realize this. Yeah. It happens in my own family, you know, I can, when someone hears it from a doctor, it just carries more weight.
And so we call base, uh, we do, we expl, Ross answered the phone. We did a job, our job explaining everything we had done. This man has decision making capacity. We’ve explained the risks up to telling him he could die. Would you please talk to him and communicate your level of concern for him? Absolutely.
Put Ross on speaker phone. The family’s listening. The patient’s listening. The medics are listening. Ross goes through, basically Ross didn’t do anything except repeat the things we had already told him. And after that, the doc, the, the patient was like. I guess I’ll go. Yeah, there you go. Yeah. And who knows if that was again, the, the hi, I’m the doctor, I’m here to reiterate that, as you said, will, but I wouldn’t give yourself any discredit there.
And maybe it needs a second time around to sink in and seeing that people are truly concerned. Maybe it was the look from the significant other who’s like, don’t mess around with this. You know, who knows what turns the tide for that individual. But I, I hear what you’re saying and, you know, in that same self-reflection, I think my areas, uh, where like Ross, I’ve been less than, um, less, less than, you know, a communicator that I would not want to have a recording played back to me of, uh, is in those times where I’m not sure what the direction is going and, and when it is like I am looking for X, Y, or Z.
I just wanted to bring it back to that thought because as you know, EM, providers. I think of that, that’s a kindred to when we’re calling cards, right? Hey, I have a patient I think is gonna need stress test tomorrow. Here’s a story, you know, I have X, Y, or Z who I think is gonna need grafting, uh, hello vascular X, Y, or Z.
And so having that structure, having that shared mental model, if you’re finding that that’s not the case in your communication with your EMS personnel, you know, what’s your relationship with your EMS director and what are, what are you doing? What are they doing? What is your system doing to try to develop that same modeling?
And so I, um, I recognize and appreciate, and I think it’s actually easier for us to understand as EM providers when we hear this experience because it’s so shared, right? Specialty service with whom we’re communicating doesn’t know our environment, doesn’t know what we’re dealing with, and we have to convince them of X, Y, or Z that we want from them, basically.
Right? And so if we can help teach or structuralize or understand that and educate, uh, our par, our EMS personnel, but like that’s fantastic that you did this. Can you lead for me with the, with the, I’m looking for a refusal ’cause I listened to that three minutes of confusing family story and now I understand as to, you know, why you’re calling me so helpful for me.
I also am curious your guys’ perspective or opinion, if I could get a little bit more specific in the space of doing or not doing things right and coming back to that idea of mental modeling. So, you know, the post Rosc COPD patient intubated getting call for that and they’re saying, you know, decreased breast sounds on the 📍 left , we’re gonna move forward to with needle decompression.
You know, asking or thinking about, okay. One of my areas of question or concerns is, you know. During this often we’re right main stem. Do you guys feel comfortable with pulling back without risk of extubation and reassessing breath sounds before proceeding to that? That idea makes a lot more sense to me now that I’ve had this conversation with you two fine fellows rather than blah, don’t, don’t start needle decompressing this post rocks person.
Like you’re probably just right main stem. So, uh, thoughts about that or how, how one can communicate, uh, such things to the pre-hospital space and what, diving more specifically in that area of like why we might want you to do less, if that makes sense. I mean, the way you approach it, I think you phased it perfectly, was in the form of a question, uh, that expresses like, do you feel comfortable with this?
Their comfort level and expresses your concerns and your mental model. Mm-hmm. Um, and so I think if you’re gonna do it, uh, that is the perfect way to do it. And, and like Will said, you know, using the clinician as a tool, as a resource is, is something that can be very beneficial to you as the EMS clinician in the back of the ambulance and to the patient in front of you.
And so, um, not being afraid to like use that I think is really important as a paramedic. Um, if you’re being asked to do something maybe less aggressive than you want to. Yeah. I, I, I think about back to something we talked about earlier, just being respectful and being, wanting to be treated like. You know, a colleague in a sense.
And so mm-hmm. If that physician on the phone says, you know, as I’m, I’m not there, but as I’m listening to this, I, if it were my patient in front of me, I would be concerned about Right. Main stem. I’m just curious about your tube depth before we go ahead and needle decompress this patient. I like it. I like it.
Thank you. All right. Just a little more confirmation of these ideas and processes and the, the model is what matters, right? Because we’re never gonna, uh, role play all of the potential craziness of your lives, our lives. And so thinking, here’s my, is this within your ability and scope? Here’s my mental model, here’s my question.
Even that simple, the structure is super, super helpful. So, all right, I’ve had your guys’ ear and your thoughts and opinions for a while now. If it’s all right, I’m gonna try to wrap it up, do a little summary and have you guys, uh, supplement that. Does that sound all right? Sounds good all right, so we have Ross and Will here who are experts in this space of, uh. EMS preparedness, um, you know, with Will being a medic and Ross being EMS Control as well, director and the creators of the Loud and Clear podcast, working with EMS personnel in that space, as well as in your other, uh, areas.
And we’ll have links to the amazing work you do in creating communities of shared experience and progress to avoid some of that skill decay and make sure that people feel. Ready for their, not just their initial couple years as a medic, which is certainly a focus that shaky ground and green behind the the ears, but also losing that fear of skill decay, knowing that you have a community of providers like you guys have created to keep your skills up.
And so with your expertise, we dove into kind of the areas of preparedness, communication, and expectations. Uh, first asking you guys about what’s it like as a medic, what are the expectations in preparedness to keep up a certain number of reps for recertification, for, you know, credentialing within your organization?
And unsurprisingly, it’s regional specific and it’s variable. Just like we as EM providers have, right? It’s gonna depend on your institution, it’s gonna depend on your environment, and a lot of it in the end sounds like it’s gonna depend on you and your colleagues. Are you guys and gals willing and able to keep your skills up so that you’re ready for whatever comes through the door?
’cause accrediting bodies aren’t gonna be the ones holding the ownership there. Then we kind of went into communication and asked, my first area was, is there a structure that all paramedics are taught in paramedic school? And will said no, basically, right? There’s a structure that we can talk about, like the leading with the punchline, talking through a specific, um.
The important points, but a lot of the education there comes in your, uh, field work and the area that you’re practicing developing skills specific to either the agency or the region with whom you’re gonna be growing as a paramedic. And then finally, we talked a bit about expectations, kind of on both sides of the spectrum, whether it be, can I ask them to do something that is, or, you know, that’s more aggressive than was the initial report or request, uh, over the phone or radio.
And then what about doing less about asking them to do less, spend less field time, do you know, maybe not intubate, maybe not needle decompress. And the example we had, and I really like the idea of the mental model, understanding where they’re coming from. Explaining your thoughts and mental modeling and then adding with that as a question, understanding you’re not there.
So you’re giving the final determination to that medic with whom you’re asking or working. How’d that go? How was my summary guys? That was perfect. Yeah. Great. Anything to add or augment or otherwise? Uh, we’ll make sure that we have all of our in audio files and references in the show notes, but I appreciate you guys coming on.
It was a blast to have you guys here and really pick your brains and think about how I, uh, communicate. I have a lot of opportunities for improvement in, you know, thinking about the cases that I’ve gone through and I know I learned a lot. I’m sure our listeners did. So thank you guys for joining me. Yeah, thank you.
Yeah, thanks so much for having us.
Keeping your skills up in rare procedures is a battle you don’t have to fight alone. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off
The Skill Decay Problem No One Talks About Enough
Both EMS providers and emergency medicine physicians face a shared, often unspoken challenge: staying sharp on critical skills between high-acuity calls. For paramedics, the problem is compounded by sheer volume asymmetry — an ER physician may see 20-30 patients a shift, while a paramedic might see six or seven. And yet the time-sensitive nature of those calls doesn’t diminish. Urban systems are too busy to train; rural systems have the time but lack the resources. Either way, the burden often falls on individual providers to self-maintain.
Key points:
–Skill decay is a universal challenge in both EMS and EM regardless of department size or geography.
–Quarterly self-assessment checklists and agency-run procedure minimums are practical tools to stay ahead of competence loss.
Communication Training in EMS: Inconsistent by Design
When it comes to how paramedics learn to communicate with receiving hospitals, the honest answer is: it depends entirely on where you train. Some systems require phone contact with a physician on every incoming call; others only expect notification for critical patients. The formal structure of that communication — whether it’s SBAR, IMIST, or something else entirely — is often left to field internship mentors, many of whom pass down habits rather than principles.
Key points:
–There is no universal standard for EMS-to-ED communication training across the country.
–The quality of communication habits a paramedic develops is highly dependent on who trains them and where.
ER Doctor Presence at the Handoff
Research and a joint position statement from nursing, EMS, and emergency medicine organizations are unambiguous: the full care team — physician, nurse, tech — should ideally be present at every EMS patient handoff. Recognizably, this cannot happen all the time. But should happen at least for all our critically ill patients. The reason is simple but underappreciated. Paramedics carry information that will never be available again: what the scene looked like, what bystanders said, what was in the refrigerator. Once that patient is in a room and the crew is rolling out, that context is gone.
Key points:
–Paramedics possess scene-level intelligence that can change diagnoses, prevent errors, and accelerate care.
–A physician’s presence at handoff is not a courtesy — it’s a standard of care backed by a multi-organization joint position statement.
Structured Handoffs Are a Good Start — But Rigidity Is a Risk
Tools like SBAR give paramedics a scaffold for organizing a report, but rigid adherence can backfire. The most critical detail of a call — a DNR, a mechanism of injury, a patient’s refusal — may not slot neatly into step one or two. Waiting for the “right” section of a structured handoff to disclose that information can bury the lead and force the receiving team to rebuild their entire mental model mid-report.
Key points:
–Structure helps recall, but flexibility is essential — don’t let a format prevent you from front-loading the most critical information.
–Lead with what will immediately change the physician’s preparation or decision-making.
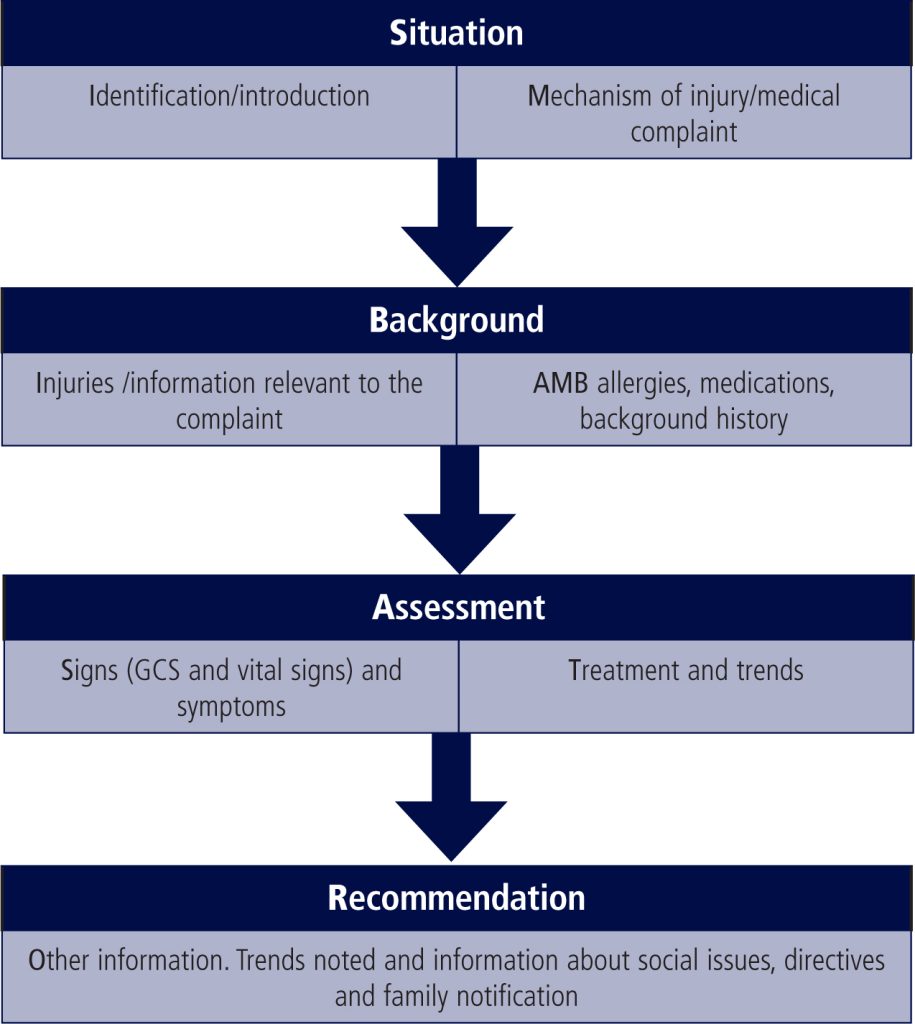
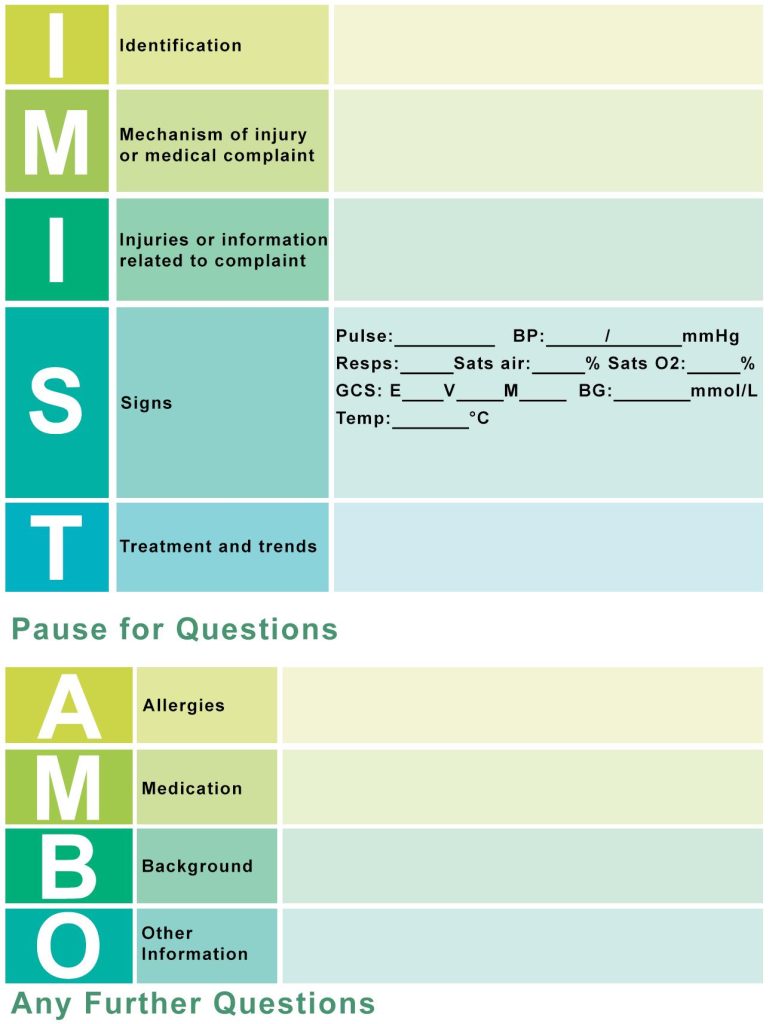
Confidence Is Not Arrogance — And Doubt Is Not Weakness
One of the most important and undertaught skills in EMS communication is the ability to convey confidence in what you know while being transparent about what you don’t. Saying “the pulse ox read as 65% — we did not have a good waveform” is more useful and more honest than presenting a number without context. Paramedics operating alone in chaotic, resource-limited environments deserve to be heard with grace — and the language physicians use to ask follow-up questions matters enormously.
Key points:
–Expressing uncertainty is a sign of clinical maturity, not incompetence — “I’m not sure, but here’s what I observed” is always better than false confidence.
–Physicians should hold questions until the end of the report, ask clarifying (not accusatory) questions, and frame follow-up with phrases like “what was your degree of confidence in that reading?” rather than “were you sure?”
Online Medical Control: State Your Ask Before the Story
When a paramedic calls for an order or guidance in the
field, the most common failure is leading with a narrative before stating the
purpose of the call. A busy ED physician is interrupted every 17 seconds and
needs to immediately orient to what kind of thinking is required. “I’m
calling for an order for amiodarone” primes the physician to filter
everything they hear through the lens of what they need to know to approve that
order. Without that anchor, the physician is just collecting information
without knowing where it’s going.
Key points:
–Always open online medical control calls with your specific ask, then provide the clinical picture, then restate the request at the end.
–If you’re getting “just bring them in,” it usually means the shared mental model wasn’t established — not that the physician is dismissing you.
Feedback, Respect, and the Long Game of EMS-ED Partnership
The best EMS-physician relationships are built on mutual curiosity and a willingness to give and receive feedback. Something as simple as “good call on that intubation decision” after a tough run builds more relational equity than months of clinical interaction without acknowledgment. When constructive feedback is necessary, the principle of praising publicly and critiquing privately applies here just as it does everywhere in medicine. Paramedics working alone with limited tools, in chaotic environments, want to be seen — not just offloaded.
Key points:
–Brief, genuine acknowledgment from the receiving physician (“good job, I would’ve done the same”) goes further than most clinicians realize.
– Intentional relationship-building between EMS crews and ED teams, through ride-alongs, shared trainings, or even a quick debrief after a tough case, pays dividends in communication, care quality, and mutual respect
Conclusion: The Space Between the Rig and the Room
The gap between the field and the emergency department isn’t just a physical one — it’s a gap in understanding, in language, and too often in mutual respect. What this conversation makes clear is that the best patient outcomes don’t happen because one side of the handoff was perfect. They happen because both sides showed up curious, humble, and committed to building a shared picture of the person in front of them. EMS providers bring irreplaceable scene intelligence. Emergency physicians bring diagnostic depth and the resources to act on it. Neither works as well without the other. Closing that gap doesn’t require a policy overhaul or a new certification — it starts with a physician stepping to the bedside for the handoff, a paramedic leading with their ask, and both of them treating the exchange as the clinical event it actually is. Loud and clear for the room isn’t just a good title for a podcast. It’s a standard worth holding ourselves to — every call, every shift, every time.
Acknowledgment
We want to extend our thanks to Will and Rob for coming on the podcast to discuss how we can be the best providers we can be and interact with our EMS-EM colleagues as smoothly and successfully as we can.
You can check out more of their podcast and work at The Loud and Clear Podcast where they offer not only amazing podcast education but also a community of providers, individual coaching, and online education.