Joint Ventures: Atraumatic Knee Pain in the ED from the Orthopod's perspective
Contributors: Robert Parisien MD and Jason Hine MD
Navigating through the nuances of atraumatic knee pain can be challenging for healthcare providers, especially in the fast-paced ED. The latest episode of the SimKit podcast offers valuable perspectives from Dr. Robert Parisien, a seasoned orthopedic specialist, and host Dr. Jason Hine, who explore comprehensive approaches to diagnosing and managing atraumatic knee pain- both in the ED and after they are seen acutely.
Transcript
atraumatic knee pain pod – 2026_01_05 19_45 EST – Recording
Jason Hine: [00:00:00] Hello everybody. Hello. Hello and welcome
back to the SIM Kit podcast.
Today we’re gonna be talking about atraumatic knee pain in the
emergency department. Something that if you’re practicing in the er, you’re
gonna see, you’ve seen it time and time again, but there’s a couple nuances.
There’s a couple specific questions that I wanted to get, some expert
consultation, some advice, and we are joined today by someone I’d say.
Is overqualified to be a guest here with us in Dr. Robert
Parisian, who also happens to be a good friend of mine, a med school buddy. And
so it’s great to have a familiar face, an old friend on the podcast. But for
those who don’t know you, Dr. Parisian, tell the listeners a little bit about
yourself.
Robert Parisian:
Well, I first want to just comment, uh, as you were saying, so Dr. Hine and I
go way back to medical school, which is, uh, quite a ways now. It’s a few, it’s
a few gray hairs on both sides here that weren’t quite there back then. I
always like, even though I’m a bit older, I always like to [00:01:00] say that he’s catching up on me. Uh,
Jaso Hine: I am, I
think, uh, I’m definitely older now than when we met.
You were, and I thought you were old back then. So what does
that say?
Robert Parisian: I
was old back then.
Jaso Hine: Yeah.
Robert Parisian:
Shows you. I’m even older now. But no, I, it’s wonderful to be here. Uh, Dr.
Hine, I really appreciate it and I can say to everyone who. Has hopefully been
following this podcast and that continues to follow this in the future.
Uh, what you’re doing truly, uh, is revolutionary here and it’s
so valuable, uh, for trainees and it’s also valuable for attendings who aren’t
utilizing, you know, all of these procedures on a day-to-day basis, which is
some of what we do in medicine. And I think to also have subspecialists on like
myself and others to talk about certain topics, um, is helpful because, you
know, we need to continue learning in this, uh, medical environment and
community and how better to do that, uh, in today’s day and age is via podcast
and getting, you know, an interdisciplinary conversation going.
Uh, also I do want to say to [00:02:00]
everyone, uh, that this gentleman here, having known him for, uh, as long as I
have, uh, and all the people that I’ve encountered in medicine, I can say is
one of the kindest, one of the most caring. And one of the most compassionate
people that I’ve ever met. And uh, I’m not just saying that ’cause I’m here on
his podcast.
Uh, that is the truth. And so, um, I’m looking forward to our
discussion tonight.
Jaso Hine: Well,
thank you so Dr. Parisian and probably ing, hopefully it’s not coming across on
camera too much. Thank you for the kind words. Um, and thank you for talking
about me. Tell me a little bit about you, tell us about your background and why
you’re the right person to talk to about this topic.
Robert Parisian: A
little bit about myself. So I’m from, uh, I’m from Maine, small town in Maine
called Bedford. I was an athlete growing up and I had some injuries back in the
day, uh, and some surgeries and some great orthopedic surgeons that took good
care of me and got me back to playing. And so that was the really the impetus
when I was about 14 years old to wanna pursue a year, uh, career, specifically
in orthopedic sports medicine.[00:03:00]
Um, and so I did that and, uh, and through the pathway, I met,
uh, Dr. Hein, uh, at Tufts for medical school. And I went on to Boston
University, did my, uh, orthopedic surgery, uh, fellow, um, residency at Boston
University. Did my first fellowship, sports medicine and complex shoulder
surgery at Boston University.
Uh, then went on and did a second fellowship focusing in sports
medicine. Really cartilage, uh, restoration, uh, cartilage repair, which is
more, is is the big workhouse, really is the knee. We’re doing some in the hip
as well. Um, but really the knee. So I did a lot of that at, at, uh, Penn, and
I was a team dog for Penn Athletics at that time.
And then I did my third fellowship, um, at Harvard, uh, and hip
preservation. So one year fellowship and hip preservation that really ended up
being a Boston Children’s Hospital in, uh, new England Baptist. And then now,
um, I’m in sports medicine practice at Mount Sinai Health System in New York
City. My practice is really, uh, shoulder, hip, uh, and knee, uh, sports
practice.
Fantastic.
Jason Hine: So, no,
no more [00:04:00] fellowships. Three. You
think three was enough? You sure about that? Well,
Robert Parisian: two
traveling fellowships after that. We could talk about those if you’d like.
Jaso Hine: No, no, I
think we’re we’re, the message is received. You are an expert among experts in
the area, and thank you so much for being a qualified individual person to
bring on the podcast for our listeners.
And, you know, again, just great to have you on board and have
such a familiar, handsome face on the other side of this podcast. So, Bobby,
Dr. Parisian, Robert, thank you for joining us. Um, all right, but we’re not
here to compliment each other. We’re talk about the old times. We’re here to
talk about atraumatic knee pain.
Now this is so common, as I said, in the emergency department.
So what I wanna really talk about a bit is. One, our history, two exams,
because I have an exam, we’ll go over here and I think it’s probably akin to
what many of us, you know, the Jack Jacks of all Trade emergency medicine docs
are doing. And then talk a little [00:05:00]
bit about our workup and our follow-up plan.
So it’s to, obviously we wanna hit the, you know, things we
don’t wanna miss. Right? The don’t miss diagnoses. That’s our job as er
doctors. And we’re gonna talk about septic arthritis and, and the likes. But to
be a good provider, to be a comprehensive care physician, we wanna do more. We
want the care to be accurate.
We want to avoid things that are wasteful. If we are doing any
of that and add value to our consultants who are gonna be referring or we’re
gonna be referring to, uh, so that they are ready to take optimal care, not
have to repeat tests or do tests that we simply negated ’cause we didn’t know
we should do it.
How’s that sound, Bobby?
Robert Parisian: That
sounds great. I would say that no matter where you are, especially though if
you’re in a community setting. Get to know your, your, uh, subspecialists that
you may be referring to. And if you are in a community, let’s say in Maine,
where I’m from right now, where I practice now, where I’m from, you can
certainly get to know who your orthopedic surgeons are, your [00:06:00] neurologist, your neurosurgeons, your
cardiologist, and get a sense of what they may, uh, want as far as some sort of
a workup.
Or do they want you, the patient seeing the pa or when do they
think that patient should be bumped up? So really communications and getting to
know, uh, that team and that environment that’s serving your community. I would
say I still do that in New York City even so I, I know my colleagues who are my
physiatrists and we discuss constantly.
I actually train their residents to teach them things in ways
in which I would like a patient to be worked up and what sort of imaging I
think they should have. And so just, I guess generally speaking, before we get
into some details here, have those conversations. Get to know the people in
your community and, and understand, uh, how they, uh, would like to see a
patient worked up.
And, uh, and have those conversations regularly.
Jaso Hine: I like
that. I like that little pearl right off the bat about how we communicate, how
we interact in the hospital, outside the hospital, having those relationships,
knowing what they look like, knowing their voice. When we [00:07:00] see ’em in the ER asking, Hey, how’s that
person doing that I sent over to you?
And being able to get that feedback right, because there’s
obviously gonna be nuance and variation of care. We’re gonna give you strong,
you know, well-founded education based recommendations here, but you might find
your orthopedics, say, Hey, stop ordering that test on that synovial fluid, or
Please get this if possible, further follow up with us.
And so having that collegiality is just gonna be huge in terms
of the quality of care that you offer and making sure that everybody’s on the
same page.
Robert Parisian:
Things change. You know, there’s reasons why there are, there are
subspecialists and you, and you can’t, I mean, it’s even difficult for us to
keep up with all the literature that’s coming out.
Um, but it’s really challenging for an, an ed specialist, uh,
to keep up with all of the literature across all of the subspecialties. So
things might change and things might adapt in time as, as they do. And so it’s
good to be aware of that and that’s, that’s also could be, uh, could be helped
by having those conversations and those relationships with your subspecialists.
Jason Hine: Good
point. [00:08:00] Good point. Thank you. All
right, so I wanna frame our conversation today around like a typical case,
stuff that we see. Time and time again in the emergency apartment. So let’s
paint a picture. Uh, John, John here today, John, he’s a 58-year-old painter,
right? So he is up and down, he is on his knees, he is working the trim, he is
doing those things.
Comes into our ER with three days of right knee pain. This
isn’t totally new to him. He says, yeah, my right knee’s my bad, right? I got
the good knee on the left. My right knee’s, the bad knee. It acts up on me from
time to time, but it’s really never been to this degree and it’s never really
lasted more than a day or two.
Today’s day three, it’s more than typical and it’s la you know,
more intense, lasting longer. Took a little bit of, uh, Motrin. He’s often
usually back at it after that. He’s tried that obviously and it hasn’t really
done a lot leading to him coming to the er. Uh, background history for him, you
know, he is got some mild hypertension.
He takes lisinopril regularly. That’s doing pretty well there.
You know, he’s a [00:09:00] classic American.
He is, got a little bit of obesity with A BMI of 42. He’s working with his
primary care doctor to drop some of those lbs. But otherwise he’s a pretty
healthy guy. Omit, kind of putting his head to the ground.
Yeah, I do smoke a pack per day. I am working on that too. But
otherwise, that’s his story. So off the bat, Dr. Parisian, anything else we
need to know about John the painter?
Robert Parisian: Well
in these scenarios, you know, first of all, when you’re atraumatic, you really
want to drill down because many times these aren’t necessarily atraumatic Hmm.
In a sense they haven’t had a car accident, they haven’t had an
injury that they can point to and say, yes, yesterday I twisted and I felt this
and this popped, or something like that. Sure. However, they might say, well,
you know what, I’ve been working a lot lately and I’ve been up and down on this
ladder for the past three days, way more than I ever have.
Or I’ve been on my knees, you know, a lot more, you know, on
this current job that I’ve been on, or I’ve been playing pickleball recently
that I picked up and I’ve been playing, you know, I played six hours [00:10:00] yesterday. I played 12 hours a day before
that, and before that I didn’t play any pickleball. So, you know, these are all
a level of trauma that, in this patient that you’re describing, this sort of
middle aged patient.
Um, so I’d, I’d wanna know what their activity level is at
least, or anything change in their activity level recently. Now from an
orthopedic standpoint, when we’re talking about joints and we’re talking about
musculoskeletal problems, it’s always where is the pain? How does the pain, how
is it reproduced?
When do you notice it? Is it, is the joint swelling, is it not
swelling? Things like that.
Jaso Hine: Sure.
Yeah. So like our P-Q-R-S-T kind of elements of the pain, and I like that sort
of either repetitive injury or microtrauma based stuff that we really should be
pinning down the patient on a little bit more. So awesome.
All. So we got some of that in information from him. He did say
up and down on my knees, back and forth, maybe non-specific about where it
hurts. You know, he touches the front of the knee as the area, it kind of hurts
all over. Um, but let’s get into [00:11:00] his
exam, right? Media the matter there a little bit. So, when assessing atraumatic
knee pain, I have a pretty, I don’t know if it’s rudimentary, I’ll, I’ll lean
on you, Dr.
Ian for this, but it’s a pretty straightforward exam.
Neurovascularly, I’m gonna be looking for that DP and PT pulse. I’m gonna check
their sensation on the medial and lateral aspect of the foot in the sandals
gap. Make sure they can Dorsey implant our flexion of the ankle and the great
toe that you know, I can do that in 15 seconds or less.
Really with the patient. Then onto the knee specifically,
obviously I’m gonna feel a bit above, feel the calf, feel the thigh. But for
the knee joint itself, I’m looking to see obvi, you know, is it warm, is it
erythematous? Is there any area of skin breakdown or overlying cellulitis? And
then. Looking for that effusion.
You know, if I’m not sure if we’re talking about someone who’s
got a little extra weight on them, I might grab that ultrasound just to confirm
if an effusion is present. And then stability exam, right? This is a big part
of what we [00:12:00] do and way bigger part of
what you do. So this is my approach, ACL and PCL.
I’m doing a lockman test for varus and valgus stress. I’m gonna
do that so I can get my MCL and my LCL. And then I’m doing that McMurray side
to side feeling for the click pop or, eliciting pain for the meniscus. And
that’s, that’s my exam. So Dr. Pre, what do you think about that?
Robert Parisian: So
again, I’m gonna go back to.
You’re in the emergency department, and I tell this to patients
all the time when they come in and say, well, why didn’t they get the MRI
there? Why didn’t they do this there? And I say, their job is to make sure that
your knee is not infected, that you don’t have a fracture that’s dangerous to
walk on, um, and that you’re safe to go out.
Into the world the next few days and with an orthopedic
follow-up to maybe get more detailed information as to what might be going on
and other, other management issues. So the everything you just hit on there is
the things that I would absolutely be looking for, especially in the emergency
department.
Clearly you don’t wanna miss a septic knee. [00:13:00] Uh, you wanna make sure that you wanna see
if there’s an effusion, if there’s a large enough an effusion, uh, that you can
aspirate that knee. I would say yes, aspirate that knee, set it off for fluid
analysis. I’ve been, we can talk more in detail about what we’re gonna send
that off for, but it’s really cell count, uh, crystal analysis as well as gram
stain and, um, and culture.
Uh, and then, uh. Outside of that, um, you’re getting into your
exam and I wanna make sure, do they, do they have a patella tendon rupture?
They have a quad tendon rupture. It’s over the age of 45. More, more likely
quad tendon. If it’s younger, it’s patella tendon. Even though it’s atraumatic,
I’ve seen things or you’ve heard stories and you know, things come in and, and,
uh, and they have these things that you would not expect.
So, basic stuff, um, I’m, I’m laying them down now on the bed.
You wanna put ’em in shorts. You want to visualize the knee. Don’t do these
exams and sweatpants and jeans and things like that. Get ’em in shorts. See the
knee, see what the skin looks like. If there’s any skin breakdown over there, I
mean, all the basics that we learned that we, that we often [00:14:00] forget, and I will still do all of this in
my clinic every single day.
Why? Because a lot of it’s practice too. You’re not gonna be
able to identify a ligamentous lax knee if you have an examined thousands of
knees and you haven’t done that exam. So don’t just do it when you’re in, when
you’re, when you’re looking for it, do it in every single knee that you examine
and have, have some sort of a system like you, just like you just said, you
have your system in place.
That’s your knee exam. Great. So I’m looking for that. I’m
looking at this as a fusion. I’m gonna milk that knee, see really if there’s
like a trace of fusion or not, because that’s important because if people have.
A focal defect, cartilage defect in a young patient, for example, uh, they
might have swelling if they have some diffuse kosis in a compartment, let’s say
in this 50-year-old, which would be the more common thing, then they could have
some swelling associated, uh, with that and some overactivity that is not
necessarily a septic knee.
Now I’m gonna have them range that e I’ll range it passively,
so I’ll lay them back completely supine. I’ll milk that knee to see if there’s
any swelling. I might have ’em push their kneecaps into the table just to look
at, uh, quad strength, see if the, the [00:15:00]
symmetry, if they have some significant quad atrophy on one side versus the
other side.
I’m hopping into a straight leg raise, lift the leg up off, no
patella tendon, no quad tendon rupture, extensor mechanisms to completely
intact. Then I’ll see if it’s completely straight. Then I’ll take the, the, uh,
the patella and I’ll just translate it medial and lateral, see if that causes
any pain.
Palpate medial and lateral as well. Sometimes people have
instability there. I’ll see if they have increased translation or
hyperextension if they have a, a ligamentous laxity issue. Now, again, this is
getting more detailed musculoskeletal examination, but this is, you know, the
exam and how I approach it.
Um, then I would, then I would, as, as they’re in that extended
position, I would then do my lockman, um, right. And so you’re looking to see
if you have any laxity and really. In a lock when you’re looking if there’s a
solid endpoint or not, it’s gonna be tough to tell if it’s less than five
millimeters or five to six millimeters, but you wanna see if they have that
solid endpoint on your lockman examination.
Then I flex ’em up. I’ll, I’ll palpate the medial lateral joint
lines again, [00:16:00] asking them, does this
hurt here? Does this hurt over here? Is it hurt when I push along the MCL? If
you’re a pickle baller, that hasn’t played in a long time. It is very common,
especially in uh, middle aged to get a MCL grade one strain.
Might that patient also have a degenerative meniscus tear right
behind that, which is connected to the capsule, which is connected to the deep
MCL so that it all blends in the symptoms in that area. Uh, yes, they likely do
have a degenerative tear. So it’s, some of these things are very common. It
would be safe for that patient with a grade one MCL strain to go about their,
their day.
If you do a l ligamentous laxity test of vari and val stress
looking at your M-C-L-L-C-L, you don’t have any laxity there, then you’re safe
that they don’t have a major MCL or LCL rupture. And this is all done with the
knee in extension. Now I get it up inflection at 90 degrees. See if they have a
SAG sign, meaning when you get it up in 90 degrees, this is the femur, this is
the tibia, the tibia sags back.
You’re concerned that you might have a PCL injury there. Could
it be a chronic injury? Fine. But these are all things that you’re [00:17:00] looking at. And what does that mean?
Typically, the, the, the tibial plateau, interi tial plateau is gonna sit
slightly anterior to the femoral condyles and it needs inflection.
And so if that, if the tibial plateau, the anterior tibial
plateau drop. Posterior to the fem, to the femoral condyles. You’d be concerned
for a PCL injury, you know, okay, again, it could be a chronic one, but at
least you’re gaining it, you’re gathering information. Now, when I get in the
90, I’m palpating the joint line, then I’m doing my anterior posterior drawer
testing.
And you gotta know where the tibia sits, um, sits in its native
position because you can be fooled if you have a, if you have a ligamentous
injury, you can be fooled to think that you have too much anterior translation
when actually you’re really starting to posterior, ’cause you have a PCL
injury, so you’re doing the anterior posterior draw.
Then I’ll get ’em up in flexion to see if they flex all the way
and see if there’s any issues with flexion. Now you’ve already ruled out septic
knee, right? So you’re not, a patient with a septic joint is not going to allow
you to maneuver the knee around this, flex the knee up like that. If I, if I
say, is a patient to my residence, if they call and there’s a concern for
septic knee and [00:18:00] I say, is that
patient walking?
Are they flexing their knee past 90 degrees on their own?
Comfortably That knee’s not septic. Okay. Low, low chance of being septic,
let’s put it that way. Um, so then I’ll get ’em up inflection, and like you
said, I’ll do the, I’ll do the McMurrays. And what are you doing with the
McMurrays? You’re really putting your hand over the anterior part of the knee.
You’re putting your fingers on the, on the anterior, on the,
uh, lateral and medial joint lines. And then you’re doing urray. So you’re
doing your valgus internal rotation, you’re doing your various external
rotation, and you are seeing if you can elicit pain in that patient or if you
can get that subluxation of the meniscus.
That’s not gonna happen that often, especially in this patient
who is got A BMI of 42, for example. That’s gonna be challenging to assert, but
again, part of your, part of your testing armamentarium.
Jaso Hine: All right.
That’s great. And it’s, it’s a lot of information in there, but if you break it
down, there’s not that much to that.
Um, it’s good, good to go back and think about history and
think about our, our tendons, right? So if this guy was just put on steroids
and Cipro for A-C-O-P-D exacerbation, that’s gonna change our pretest [00:19:00] probability for some of these things. And
an important history to get. I wanna, so one to summarize, I like, we start in
the ex extended position, we see if they can do a straight leg raise and then
you’re doing your lockman that their
Robert Parisian:
mechanism is intact, so that rolls that out.
Jaso Hine: Those two
parts are out right away. Yeah. And you’re doing your lockman extended. And
then help us differentiate the extended lockman test
Robert Parisian: and
well not extended. So you’re doing it slightly, the lockman, you’re doing it in
slight flexion. But my point is I’m not bending and not putting him straight
doing this.
You can do all that. That’s fine. I have ’em extended. I’m
gonna do it, uh, medial lateral translation of that patella. I’m gonna, I’m
gonna palpate the medial lateral patella facets. If it’s a young patient that’s
active, they might have full, uh, focal caral defect there. Um, and then I’m
gonna slightly flex them as you would a typical lockman and do the lockman.
But my point is it’s all kind of stepwise where I’m sort of,
I’m kind of in this extended knee position and then I’m gonna flex ’em up.
Palpate the joint lines anterior posterior drawer. I, I’m also gonna do various
AAL laxity testing with it extended as well. Then again, flex stop to 90 do
that, and then I get ’em [00:20:00] all the way
up collection and then I do the McMurray’s.
And so it just makes for a, a more efficient examination. And
that’s just kind of floats through that way.
And if it’s painful to ’em, I’ll say, is this your pain? Is
this why you came into the emergency department today? Right here where I’m
pushing? Yes. Okay, great. So then they might have peasant around bursitis,
along the bursitis, thinks they might have pre patella bursitis. This patient
right here, uh, a plumber, a carpenter, a active individual like this who’s on
their knees not, uh, uncommon to pre patella bursitis.
So bursitis right over, uh, the patella. And so again, it’s,
it’s a matter of examining that, seeing exactly where they have pain and these
things, they’ll point exactly in that spot. Or if it’s patella tendonitis, they
will point exactly on their patella. Tend, this is where it hurts, where it’s
when I go up and down stairs hurts when I’m trying to stand from a seat of
position.
Jaso Hine: They’ll
notice it that way. Okay. I’m gonna help pin down one element for me in
clarification. [00:21:00] And if there’s,
they’re testing the same thing in different ranges of motion versus different
testing, the slightly flexed lockman and the fully flexed anterior, posterior
drawer. Is there different elements to that, or why are you doing both?
Robert Parisian: Oh,
so the lockman is gonna be the one that is going to be sort of the gold
standard or the pivot shift. And so I, I didn’t get into that. If I’m really
concerned for an ACL, I’ll do a pivot shift. Okay. So that is where you
internally rotate the tibia. You gonna place a valgus force? Okay. And you’re
gonna go from flexion to extension, and that’s gonna reduce, the IT band is
gonna pop, is gonna shift that and pivot that and reduce the tibia back
underneath the femur.
So when you’re in the flex position, the tibia is gonna be
sublux anteriorly, internally rotate valgus and extension, and it’s gonna, and
then the t the it band will reduce that tibia back underneath the femur. And
that’s a positive pivot shift for an ACL injury. But it’s like anything else,
instead of [00:22:00] relying on one
examination, you have a couple different ones to help you.
Got it. So really the, the, the ACL examination is gonna be a
lockman anterior draw and a pivot shift.
Jason Hine: Got it.
Awesome. Thank you for that clarification. I think I’ve been calling my
anterior drawer lockman for probably too long, so Thank you.
Robert Parisian:
Anterior drawer, you get ’em in 90 and then you pull the tibia anterior, the
lockman, they’re, they’re slightly flex about 30 to 45 degrees.
And then you’re, and then you’re pulling and you’re trying to
get that. So it’s a slight, it’s a slight, it’s a slight flexion. Exactly. And
they gotta be relaxed. You gotta just talk with them, get ’em to relax leg. But
the one where you’re getting up in 90, you’re putting your thumbs on the joint
line, on the anterior joint line, A to see.
’cause your thumbs if you’re on the, if you’re on the anterior
tibial plateau, your thumbs should bend slightly over that anterior tube by toe
plateau. Why? ’cause again, the anterior anterial plateau should be anterior to
the femoral condyles at 90 degrees of flexion. So your pump bend right over
that tial plateau.
If you’re putting your [00:23:00]
fingers like this and you’re hitting the femoral condyle first, and that tibial
plateau is posterior concern for chronic PCL injury.
Jaso Hine: Got it.
Awesome. Thank you. All right, so we’ve examined the knee. We’ve started an
extension, we’ve done a straight leg raise. We’ve slightly flexed it. We’ve
done our lockman, we’ve brought ourselves up through d varying degrees of
flexion, doing our, uh, anterior posterior drawer, the test that you had
mentioned.
Now let’s get onto a little bit more of our workup. Our
physical exam is a huge part of the, atraumatic knee pain workup. And as you
mentioned, I really like, and I’m just gonna reiterate, focusing on any
specific, you know, thumb or finger point specific pain. It’s gonna point
toward our bursitis. It’s gonna point towards other elements, and recognizing,
you know, how that tibial plateau lines up with the femoral condyles is gonna
give us some information, at least toward what we’re dealing with anatomically.
Robert Parisian: But
as we go down with it. Sorry, sorry, Dr. If you’re dealing with a pez sarine
bursitis, you can relieve that patient’s [00:24:00]
pain very quickly with a, with a corticosteroid injection right there in the
emergency department. And that’s fine. And then they can go through, through
some physical therapy and, and, and you can help them if you have a large joint
of effusion.
If you get an x-ray, which we’ll get into that, you get an
x-ray and you have some significant joint space narrowing, some osteophytosis
and some real severe, you know, de degenerative joint changes, you might do
the, the aspiration, send it off, make sure it’s not septic. But, um, but you
may wanna hesitate on doing a corticosteroid injection at that moment because
if you send ’em to your arthroplasty specialist, they’re gonna have to wait at
least three months to do, uh, total, uh, total knee arthroplasty surgery.
Mm-hmm. And that’s fine, but you just wanna educate the
patient. You know about this. Yeah. And so a lot of the physiatrists that I
work with and I train, um, and you know, they know now, you know, if they’re
considering doing a, an injection of corticosteroid, they at least educate the
patient or they’ll contact me and say, Hey, that we’re thinking about doing
this, we’re considering doing this.
Is that okay to go ahead and do that? Just, just things to
know.
Jaso Hine: Awesome.
That’s good. I’m gonna put a pin in that ’cause [00:25:00]
we’re gonna come back to like, once we’re in the joint space, what can, and
what should we do and when should we not do it? So we’ll come back to that
topic, but, all right. Work up. So.
Outside of extenuating circumstances, you know, IV drug user or
hemo, anything like that. You know, I find general serum labs for atraumatic
knee pain to be nearly helpless or help worthless, I guess I should say. Um,
even if I think it’s gout as an example, uric acid, acid level in an acute
flare doesn’t really add a whole lot.
Sometimes it’s done. People say, oh, it’s high. Yeah. But
that’s there. But is it really meaningful in a lot of ways, uh, is a question
that comes up. So, uh, Dr. Preen, are there any serum labs that you want in a
person with this, atraumatic, traumatic knee pain? Barring any extenuating
circumstances?
Robert Parisian: No.
If you’re not con, if you’re not concerned for, uh, sepsis or any systemic
symptoms, uh, and you’re really looking for a source of that infection, uh,
then [00:26:00] no.
You know, I, I would say there’s n there’s not any, you know,
some serum labs that we would get routinely.
Jaso Hine: Okay.
Excellent.
Robert Parisian:
Because then, you know, if, if you have a young patient, if you have somebody
in the woods, right, we’re getting down to the other pathways of like Lyme,
arthritis, and there’s all these other things that you need to be concerned
about that can certainly present.
But that’s really after you roll out all the more common
things.
Jaso Hine: Fair.
Yeah. That does make sense. Um, all right, so labs, serum labs. Anyway, we will
put a pin in other labs for a moment. Not necessarily valuable, barring
extenuating circumstances. Imaging. Imaging, I have to admit. In my, atraumatic
knee pain patient, especially as they get in advanced years, things like that.
I will on occasion or frequently get a plain x-ray on these
guys and, you know, uh, if there’s a risk for a cancer or something like that,
you know, we have our pack per day smoker. Sure. Maybe there’s a pathological
lesion. Maybe I’m justifying it that way, looking for the osteolytic. But I
also make myself feel better sometimes saying, well, our [00:27:00] orthopods are probably gonna want this
plain film X-ray, so I’ll get it.
Um, you know, is choosing wisely gonna slap me in the back of
the head, probably. Uh, but how accurate am I in getting these types of
studies? Or is there u any utility to a plain x-ray in a, atraumatic knee pain
patient?
Robert Parisian: The
physiatrist that will come, uh, to my office and, and, and train in the office
and the residents.
Um, I will ask them, how can you tell this? How can you tell
that? How can you tell this? Then we’ll get the X-ray and we’ll go through it.
So. For all my knee pain patients, I’m getting full length alignment films.
Okay? Right. So hip to hip to ankle. Why am I doing that? Mm-hmm. I’m, I wanna
see what their alignment is.
I wanna see if they have significant VARs or valgus. So if they
have significant VARs, they have significant medial joint space narrowing.
These are all helpful for me. If they have medial joint space narrowing, um,
and uh, in that vari and their middle age, they’re gonna have, obviously they
have some arthritic changes in that joint.
They’re gonna have meniscus tear. [00:28:00]
Is that going to be symptomatic or, or not? Is it going to be something that is
a bucket handle, traumatic tear? Are they gonna have an underlying route to all
these things? You’re gonna find out an MRI later also, why am I doing that? I
wanna take a look at the hip joint.
So knee pain can be referred to the hip, and especially in a
young patient, you do not wanna miss a young, heavier kid who has a scfe
mm-hmm. Slipped capital, femoral epiphysis that’s coming in. And there’s a lot
of literature out there that, uh, uh, that demonstrates that a lot of these
patients are gonna come in with, with a primary complaint of knee pain.
Mm-hmm. Now, the majority obviously will come in with hip pain,
but there is a fair amount that come in with a primary complaint of knee pain.
And so in that patient population, I would absolutely get, uh, either an AP
pelvis or you just get a full length alignment film. So you can take a look at
the hips.
Now, if it’s a, if it’s, uh, any age patient, or let’s just say
the, your patient that you have here, severe osteoarthritis of the, of the hip
could be [00:29:00] radiating down the anterior
and anter medial thigh into the knee. Um mm-hmm. That, that is presenting as
some sort of knee symptoms. Uh, they could have, um.
Osteonecrosis of the femoral head. And so that’s also
relatively common. It’s not, you know, it’s not overly common, it’s relatively
common. So they could have osteo necrotic changes of the femoral head and
collapse of that femoral head that could be causing referred pain down to the
knee. And so I’ll get that.
I get a standing AP film, I’ll get a flexed view. That gets,
allows you to look at different aspects of the femoral condyles to see if they
have an OCD lesion. ’cause many times you’re only gonna uncover this OCD lesion
and the medial femoral condyle. And a patient that you get like a Rosenberg
view, which is, which is like a 45 degree flex PA view.
So it’s not a straight AP view of standing, which I do get, but
then I flex ’em to 45 degrees. So you can see, uh, along their condyles more
and you can pick up an OCD lesion Now in the emergency department, it’s not
gonna change things significantly, but these are all reasons why, you know,
plain radiographs can be helpful
and, and why we get them.
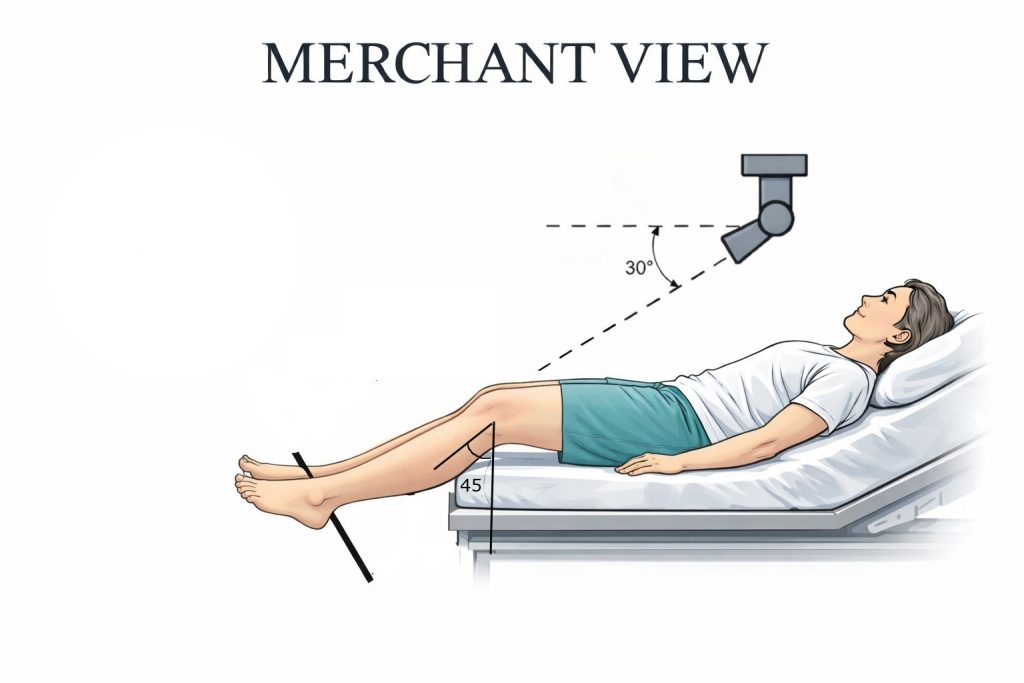
Uh, I’m also getting a merchant view, not a sunrise view, so a
sunrise view, they’re really flexed and the patella is fully engaged in the
trochlea, so you can’t see down the joint line. Mm-hmm. And so I wanna be able
to see between the patella and the trochlea. So I get a merchant view, which is
like a 45 degree or 45- 60 degree flexed view, so that the patella is at least
floating above the trochlea.
So you can see between, and you can see is there some media
lateral translation, you know, any other abnormality that’s there. Um, and then
I’m also getting the, uh, um, a lateral view, uh, to see if there’s any
patella, Ulta, or Baja or any other abnormalities. Now, in addition to that.
Yes, there are oncologic or malignant processes that we do find in orthopedics
many times ’cause people will present with some sort of joint or bone based
pain and we uncover a lot of oncologic, um, issues.
And so that is also, uh, another reason why it’s, it’s helpful
and beneficial to get an x-ray. In addition to that, like I said, I would say
that there’s so many patients that [00:31:00]
come in that say it’s matic that say they don’t remember this, they don’t
remember that, and they have a patella tend er rupture.
They have a quadin er rupture. You won’t get an x-ray, but
they’ll have a fracture potentially somewhere, you know, in that, on that
x-ray. And so, yeah, I, I think that, you know, we’re orthopedic surgeons. We,
we, uh, analyze plain radiographs. They’re extraordinarily useful.
Jaso Hine: Okay, well
that’s good information. Two things, few things, five things, I don’t know.
Uh, one, alcohol, methamphetamines, opioids are a hell of a
drug and they, trauma happens without recollection, not uncommonly. So that is
an important takeaway, especially for ER docs two. Um, the x-ray has utility,
um, and then three, I’m probably not gonna be able to get all of the x-rays
that you mentioned well and accurately.
So there’s a pretty high probability in follow-up that you’re
gonna be doing additional films to get the information you may want. Is that
accurate to say?
Robert Parisian:
Yeah. We’ll, we’ll, if [00:32:00] we are
concerned for a ligamentous injury or a meniscal injury, or focal conal defect,
then yeah, we’ll be getting an MRI and other follow-up films.
Jaso Hine: Yeah.
Well, and just in terms of the x-rays themselves, you mentioned several x-rays
that I don’t know if our ER techs will have or do perform. And so I’ll get the
list, we’ll put it in the show notes of the ones that you’re typically doing
yourself. Um, but I’m also recognizing that the films that are done in the ER
may not adequately cover all of the potential x-rays that you may gather as an
ortho cot
Robert Parisian: to
rule out what you need to rule out.
I think as far as fracture and to identify if there’s any sort
of malignant or oncologic process that’s happening there, then I would say an
ap uh, lateral and some sort of patellofemoral, which I would say would be a
merchant view. Um mm-hmm. Which should suffice with consideration of getting an
AP pelvis or a full length alignment film.
So you can take a look at the hips, especially in a young
patient. You don’t wanna miss a young person with osteonecrosis, so capital
femoral epiphysis, or other sort of, you know, hip related pathology. [00:33:00]
Jaso Hine: Yeah.
Fantastic. And that’s, that’s like board question 1 0 1 in emergency medicine
in our obese young patient with knee pain.
So hopefully we are capturing that and not thinking too much
about CFI in our, was a 50 something year old painter. But, um, outside of
x-rays advanced imaging, we mentioned briefly RI there are a few emergent MRIs
out there. Oftentimes we’re focusing on thoracic or lumbar, you know, um,
looking for any type of Cara syndrome or uh, spinal epidural abscess.
I would say atraumatic knee pain is not one that comes up
commonly as an indication for MRI, even including concern for septic arthritis.
’cause we’re about to get into joint fluid analysis. So in addition to, or
subsequent outside of MRI, are there other imaging modalities that you find
valuable that are done in the emergency department?
Robert Parisian: No
planned radiographs are really the most valuable, uh, imaging. I mean,
obviously the other one that would be, uh, common for us would be [00:34:00] a CT scan. Mm-hmm. Um, but that’s not
gonna be as commonly utilized and beneficial. That’s really for many times for
operative planning, uh, purposes that you’re getting a CT scan, not just of the
ne but anywhere.
Um, and I think with utilization, uh, and you and your
expertise in developing expertise in ultrasound, I think ultrasound can be
extraordinarily valuable. And this is something where you, the emergency, uh,
medicine, uh, physicians and our physi colleagues are, uh, utilize a lot more
often than we do. And so that, that, those things can be very helpful.
I mean, look in the shoulder, we published a study showing that
ultrasound evaluation of a full thickness rotator cuff tear was just as
accurate as an MRI. Now it got less accurate when you had partial tears and
when you’re trying to evaluate the subscap, which is a bit deeper, but you know
that the ultrasound can be very valuable.
Jaso Hine: Yeah.
Yeah, I’m glad you brought that up ’cause I was gonna just put that pitch out
there. As somebody who loves using bedside ultrasound and you have another
knee, so you can always compare and contrast if you’re wondering about tendon
injuries, ruptures, even bursitis. Ultrasound [00:35:00]
has some utility from our perspective, so I’m glad that you find it useful as
well.
All right, let’s talk about the knee effusion, which is kind of
where the meat of the conversation and actually the impetus for the podcast and
the conversation today came from. So the water on the knee, the knee effusion.
If a patient lacks risk factors for septic arthritis, you know, they’re not env
engaged in IVDU.
They don’t, uh, undergo dialysis routinely. They’re not
immunocompromised, brittle, diabetic, all the things we know. The joint is not
hot, it’s not erythematous. Is there value in tapping the joint? Um, and we’ll
break this down a little bit ’cause there’s two ways that that could be
potentially valuable. So diagnostically, is there any value in fluid assessment
or is that water on the knee?
Almost always Osteoarthritis and a simple effusion.
Robert Parisian:
Well, it also goes, it goes to your pretest probability, right? So how
suspicious are you that this is a septic knee? So if it’s this 52-year-old
painter that, or, you know, [00:36:00] uh,
worker that comes in, uh, he doesn’t have any risk factors. Uh, he is actively
and pass and you’re passively, uh, extending and flexing his knee comfortably
or, you know, maybe some minor discomfort when you get him with a deep flex.
If he’s got some patellafemoral symptoms or even medial joint
line symptoms, but relatively comfortable then and low likelihood that’s a
septic joint. Sure. Uh, if it’s, if it’s not hot, ery saw the other factors. So
at that point in time diagnostically, no, I would not aspirate the joint also.
Everything that we do, even if we think that they’re small, minor procedures
all carry some sort of risk.
And so is it possible to inoculate, uh, a joint that is not
septic? Yes, of course that is possible. So, you know, I’m really, you know,
teaching our residents that you’re gonna aspir a joint, first of all, if you
think that there’s enough fluid in there to actually collect enough fluid to be
analyzed. Um, and also do you think, and, and what is your suspicion that this
is truly a septic joint versus someone that has, you know, an effusion [00:37:00] secondary to some osteophytic changes in
overactivity.
Jaso Hine: Okay,
perfect. I like that. And I mean, I use perfectly sterile technique every time,
so it’s not gonna happen to my knees, but, you know, it’ll happen out there for
others. Um, all right, so that’s the diagnostic side. How about
therapeutically? You know, we have this guy who’s got a big old water, water
bag.
Knee. He’s got a known osteoarthritis. We expect it to be a
simple effusion. Maybe we can take some of that pressure off and relieve the
pain and then. Are we, are we, and should we be putting a little bit of a
cocktail in there? You know, different, different strokes for different folks.
It seems like the ones that I’ve seen about putting in like three mls of
lidocaine, uh, 1%, I guess the 2% is a little more, little more caustic to the
cartilage.
Uh, 0.2, 5% bupivacaine and some triamcinolone is what I’ve
seen out there. Um, so let me ask you that one. Take the fluid off to be
beneficial to the patient. Uh, yes or no. And then two, are you putting any
kind of special sauce in the knee? [00:38:00]
Robert Parisian: So I
will aspirate, uh, uh, knees or joints in general, but knees, yes, for
therapeutic, for reasons if they’re, if they’re swollen, um, or, you know, in,
in patients that have ACL ruptures, there actually is a fair amount of
literature to show that they’re really catabolic enzymes that are in that knee
that may be, um, uh, deleterious, uh, to the articular cartilage.
And so it may be helpful actually to aspirate that effusion.
So, yes, in the, in the office setting, uh, for example, I will do that, um,
for therapeutic reasons, uh, and purposes for patients. And, and of course,
you, if you can aspirate 60 to 80 ccs out of a need, it’s gonna feel better
immediately. Now, what do I do after that?
Nothing. I do not inject anything back into the knee at that
point in time. Uh, if I am going to inject, uh, then I typically inject, you
know, um, visco supplementation or PRP, uh, for the vast majority of patients
that I have, um, because the literature and the data has shown those to be the
most beneficial.
Uh, when it comes to foose, focal chondral defects or [00:39:00] some osteoarthritic changes, or just some,
you know, mild to moderate kosis. If you’re gonna do corticosteroid in a, in,
in some sort of an, um, aesthetic. Ropivacaine has been shown to be the least
chondro toxic, and so I will only inject ropivacaine, um, into, into joints.
Um, but I’m not a, I’m not. A huge proponent of corticosteroid.
Uh, however, can corticosteroid work? Can it be beneficial when it comes to
symptom relief? Of course, yes it can. There’s very good data showing that,
that corticosteroids, especially in an osteoarthritic knee, can certainly be
very helpful, uh, for symptoms.
Just let that patient know that if they’re gonna be following
up with their total knee specialist, they will not be able to do a total knee
on on you for at least three months if we do this injection. Now some of ’em
may say, that’s fine, I have no interest in getting a total knee, or, I have a
bunch of things going on in my life, please just, I want the pain relief right
now.
Fine. At least they, they’re educated on that. Or you, we will
have some that will say, oh, okay, I understand. I would rather go have that
conversation [00:40:00] with the total knee
arthroplasty specialist. Thank you for aspirating my knee. It feels a lot
better ’cause you took out 60 ccs. Um, and I’ll go have that conversation with
them and then if we determine I’m not gonna have a total knee, then maybe we
can do an injection at that time in their office with them.
Jaso Hine: Perfect.
Huge, hugely valuable por pearl for me, because I didn’t know that I didn’t,
you know, I, I’m not injecting most of the knees. I do, I’ll be honest. I’ll,
I’ll take the fluid off and, um, you know, usually call it a day. Um, if
someone is yet to establish with an orthopod, uh, we know our time to see them
and go through pre-op and get prepped for all that is gonna be longer than that
time.
Sure. I, I guess that’s a consideration. Um, but it’s good to
know that that puts a, a three month blocker on that total knee. So
Robert Parisian: the
vast, vast majority of us are three months. And so I just gave a talk, for
example, at the, uh, for American Academy of Orthopedic Surgeons. We had, uh,
entire panel and different topics on rotator cuff and, and, uh, and I did the
orthobiologics and the corticosteroid.
The point is, even with rotator cuff, if you give a
corticosteroid [00:41:00] injection within one
month prior to a rotator cuff repair. During the rotator cuff repair, or even
one month following the rotator cuff repair, all those patients have
significant increased risk for infection. Mm-hmm. And so we have similar data
across, across, uh, joints.
A lot of that is about six weeks. Many of us are waiting at
least three months to do anything within these joints. Even from an
arthroscopic standpoint. I’m pretty conservative. I’ll still wait that time
before I even do an arthroscopic surgery.
Jaso Hine: Okay. Good
to know. Thank you. So three month window on that shoulders.
I’m not objecting those knees. Good to know about. I’m gonna
bring it back a little bit ’cause you mentioned something with the bursitis,
and this isn’t in my clinical practice, but maybe it should be. So if we’re
recognizing a peasant iron or pre patella bursitis and you can do a cortico
injection, tell us your process there.
What are you using and how much.
Robert Parisian: Uh,
so for the corticosteroid injection, uh, of the peasant bursa, I’m not using
much. It’s gonna be, you know, roughly a two to one. Uh, just because that [00:42:00] space doesn’t take much and it’s not going
to, patients can feel uncomfortable, uh, in that, in that area because it’s
not, you know, you’re just injection the bursa, uh, and there’s not a lot of
soft tissue overlying that area.
But with a, but with a corticosteroid injection with, for PS
and C bursitis specifically, uh, it, it can work very well. Um, I will tell
patients you can try icing it. You can try activity modification, you know,
non-steroidal anti-inflammatories and Tylenol. The other option you don’t have
to do it is a corticosteroid injection.
Now, pre patella bursitis, you see it less, less common. Um,
and so I’m not really injecting those as commonly, um, sometimes compressive
wraps and really just staying off the knee and, uh, mm-hmm. Because the pre
patella bursitis is really one that they’re gonna be on the knee. They’re,
they’re are plumber or they have some sort of profession, you know, where
they’re kneeling off and if it’s possible because it, it’s really friction
based, right?
Mm-hmm. And that’s why they’re developing this predelivery
bursitis sometimes with the on bursitis, you know, not dissimilar, you know,
they’ll be, they’ll be, have a lot of friction on their elbow or they’ll even
bang their elbow and develop that. So I’m not really injecting those routinely,
but with the [00:43:00] peasant bursitis, I
will.
Jaso Hine: Okay. And
what are you using and how much,
Robert Parisian: oh,
okay. So yeah, it’s, you’re gonna be really just, uh, kenalog and, uh, and, uh,
whatever cocktail you, you have, it’s, there’s no really, you know, any, any
literature on our end to suggest one over the other.
Jaso Hine: Okay.
Yeah. So dealer choice. Great. Right. Um, all right, so last bit of this, we’re
talking about tapping knees.
Um, what about the old anticoagulated patient? We’re seeing
more and more of ’em, you know, they’re gonna be on 10 a inhibitors, probably
more so than warfarin. Uh, they got their Eliquis, they got their Xarelto, you
know, they got a painful joint. It’s got the effusion. It’s a little bit warm,
you know, if I find that it’s a hemo orthosis, you know, we see these joints
and we say this could be a spontaneous hemo, orthosis might not be, could be,
you know, crystal, it could be septic, whatever in that space, right?
We see the knee, it’s swollen. They’re on 10 a inhibitor
considering on differential spontaneous hemo orthosis, [00:44:00]
do you tap these joints to confirm that diagnosis? And on the other side of it,
we recognize that it’s one of many elements that could be their diagnosis. Are
we at risk for inducing a hemo orthosis in somebody that we’re trying to rule
out a hemo arthrosis?
If that makes sense.
Robert Parisian: It
makes sense. I mean, if, if you have a patient that is coming in that has a,
that has a swollen knee, and again, it goes to your pro, uh, uh, to your
pretest probability, do, how suspicious are you that this is truly a septic
knee versus the hemo arthrosis? It can be challenging, I understand that.
But if you’re concerned that this is a potential septic knee,
you don’t wanna miss that. Right? You don’t wanna miss a septic knee scenario
because obviously if the patient doesn’t have a significant severe
osteoarthritis, then they’re there. The, um, infection is gonna degrade that,
that articular cartilage very quickly.
And then you could be leading to, uh, a systemic sepsis if you,
you know, are, are leaving a systemic, uh, rather a septic joint, uh, left
untreated, right? So you certainly don’t wanna miss that. So in those patients
that [00:45:00] you’re, they’re concerned for a
large diffusion and that you’re concerned for a septic joint, I would say
aspirate that joint, um, and then send that fluid for analysis, uh, in the
patient that may be on some of these anticoagulants, I would say if they do
have an effusion, I would aspirate the joint, uh, and make sure I don’t miss a
septic knee.
Jaso Hine: Perfect.
Good. I like the simplicity of that answer and it seems pretty well supported.
If you look at kind of the literature on the topic, the number of times when
people are doing injections or aspirations and inducing hemo, orthosis is near
zero. So it always comes up, you know, something that we consider, we don’t
want to do harm when we’re trying to do good, but if septic arthritis is on the
differential mm-hmm.
Which usually it is, if you’re thinking about a, you know,
warm, painful, swollen knee, then you have to do what you have to do and, and
if you do good technique and you talk with the patient about risk, sounds like
from Dr. Parisian’s standpoint anyway, we’re good to go.
Robert Parisian:
Yeah. I mean, you know, again, an orthopedic standpoint and I think in
medicine, but you know, it is good to have data and if you’re, if you’re
concerned, you want, you want the data points, you also [00:46:00] do, you don’t wanna miss some of these things.
And the septic joint is certainly one of those.
Jaso Hine: Yeah,
Robert Parisian: fair
enough.
Jaso Hine: All right,
so we’re gonna go forward. We’re gonna tap our painter’s knee, um, may, maybe,
you know, simple osteoarthritic and we can take the fluid off and help him feel
better. We’re gonna maybe avoid our steroids so that he can see one of our
esteemed colleagues and have his knee replaced if need be.
But I’m taking this fluid, let’s say it’s still on the
differential. It’s, it’s a, uh, you know, a warm hot joint. He can’t really
range appropriately. Septic arthritis is on there. You know, we’re gonna talk
about OID disease as well, crystal arthropathy. I’m gonna get that fluid. What
am I sending it for? What are the tests that you want?
And then after you tell me your answers, tell me what gives you
your highest concern, or what are you using as your line in the sand for that
septic arthritis? Clearly we’re talking about cell count and the differential
Robert Parisian:
clinical examination, right? So you’re not aspirating again without your
suspicion and clinical exam.
Uh, and then once you’ve seen a septic knee, then you’ve seen
it and you understand what it looks like. [00:47:00]
Uh, then if you do the aspiration, you cell count, right? Crystal analysis. Uh,
and then, uh, gram standard culture. So if you have a cell count over 50,000,
that’s a septic knee. If you have, uh, neutrophils over 90% with a cell count
over 50,000, that’s a septic knee, especially when it comes with an examination
that was concerning, which is again, the reason why you aspirated.
And so that is a patient that has a septic knee. Now we do de
gram standard culture as well. Culture comes back positive. Now you can have
specific antibiotic management, uh, for, uh, that knee, but really that’s what
you’re looking for in a, in a native joint.
Jaso Hine: Fantastic.
Right down the fairway there. Now we’re from Maine.
Well, you are, but I’m a transplant. Are you sending, uh, most
of those, are you gonna be doing your tick-borne, vector-borne illness? Uh,
serologies on that as well.
Robert Parisian: I
think it’s reasonable. I think if you’re in those areas that are endemic to
these, uh, you know, different sort of, you know, uh, exposures, um, like a
Lyme for example, uh, then yes, I [00:48:00]
think it’s, it’s completely reasonable to, to send, uh, for those as well.
Because again, especially in a kid, for example, anybody
really, but in a kid, you don’t wanna miss some of these things. And, uh, and
I, and I think it’s, uh, it’s very reasonable to send off and add those, uh,
why you have this synovial fluid. Fantastic.
Jaso Hine: That I did
that two weeks ago. It was, it was the winter.
Tap the kid’s knee. It looked like numbers were concerning for
septic, but we still sent our, our vector borne pathologies because it’s still
an interesting diagnosis that can come up at any time of year, weirdly enough.
But
Robert Parisian: all
right. No, without, without question. In the vast majority of the time, as you
know, the vast majority of time it’s gonna be negative.
Okay? And so, and that’s fine. You know, it might be negative,
but a few times. And if you do it and you work long enough and you aspirate
enough, if you know knees, uh, that have effusions, it will pop up. Uh, and
you’re gonna feel glad that you, uh, diagnosed that patient because the many
weeks and months that that patient is now going to go without a diagnosis,
because they’ve already had their [00:49:00]
knee aspirated, it’s already been tested, it was clean, they’re gonna, you
know, and that, and they could have, they could have some serious problems.
And again, anybody, but of course, if you have a young patient
who has some underlying, you know, Lyme, arthritis that has not gone, uh,
diagnosed, you know, you, you’ve really saved that. Patient and that family,
um, a lot by going ahead and, and adding that to your, to your, um, analysis.
Jaso Hine: Makes
sense. I like it. Yeah.
We’re not just saying, okay, it’s not gout, it’s not sepsis.
We’re gonna leave it be, we’re still gonna keep working our way down the
differential. Mm-hmm. All right. I’m gonna do my best to do a summary, unless
you have other pointers or pearls right now.
Robert Parisian: Uh,
none that I can think of.
Jaso Hine: All right.
You think while I talk?
All right. So we have Dr. Preen here, orthopedic
extraordinaire. We’re talking about the atraumatic knee pain. We started with
our elements of the history and I actually really liked how we dove into. The
P-Q-R-S-T of the pain, trying to really localize it, figure out their
repetitive [00:50:00] trauma, their
microtrauma, their work, their profession, anything outside of their normal
activities.
I added in a little thing about, you know, making sure we’re
checking out medications that put them at risk. Obviously their social
histories gonna come into play, um, in terms of their pre-test probability for
septic arthritis, cat arthritis, et cetera. When we got into the physical exam.
I like that sort of starting an extension and working our way through.
So right, we’re gonna do our, uh, neurovascular check distally.
We can start in full extension and do a straight leg raise to look for any of
our tendon ruptures, clean, easy way to do it. Then we’re gonna put ’em in a
slight extension and do our lockman testing, sorry, slight flexion. Do our
lockman testing.
We can do our varus and valgus stressing, and then we kind of
gradually range them further and further. The pearl and tip for me here was to
identify that tibial plateau in its location compared to the, uh, femoral
condyles epic condyles to see if there’s any mal alignment there. And we can do
our McMurray and our other testing in that way.
Once we go [00:51:00] through
that physical exam, there is some utility in our x-rays, uh, for our orthopods.
So don’t feel bad if you’re getting x-rays in atraumatic knee pain. You can
forget choosing wisely. Uh, I know it’s back pain that they talk about, but can
consider that there as well. Um, for the knee, let’s come back to that.
We are gonna think about our OIC lesions. We’re gonna think
about joint space narrowing, medial laterally. There’s many x-rays that we. Are
probably not accurately going to get in the emergency department, but we do
wanna think about hip, we wanna think about alignment films. And remind me of
the term that is not a sunrise view about the patella alignment that you added
as a consideration
Robert Parisian: for
er Yeah, it’s a merchant view.
And so the merchant view is actually very helpful. The sunrise
is, is almost useless. And, and so the patella is completely engaged within the
trochlea. So even if you had so many, uh, medial lateral translation or even
lateral tilt, you’re not gonna see that. Also, um, with the, uh, with the, uh,
merchant view, you can see down the joint line.
Um, and so [00:52:00] it just
tells you a lot more information. And so even if you’re not looking for all of
those subtleties, it, it’s a better test to get in general. ’cause the merchant
view as opposed to sunrise, it’s just like in the shoulder. You want to get a
grassy view, which is a true AP as opposed to an AP view.
Why is that in the shoulder? So this is the glenoid, this is
the, the humus and the humeral head and the AP view, you’re gonna be like this
or more like this. Mm-hmm. And so it’s, there’s an overlap here. A grassy view
is a true ap. It’s turning like this and you’re seeing right down the joint
line. Okay. So you can see if there’s any posterior translation, anterior
translation that might suggest a dislocation.
And so the merchant view is similar to a grassy view on a
shoulder where you’re actually getting right down the joint line giving you a
lot more information.
Jaso Hine: Fantastic.
Thank you for adding pearls for the shoulder. We’re not on that podcast yet, so
we’ll have you back for that one. Um, but I’ll add a, I’ll add some imagery.
Uh, we’ll have the merchant view in the show notes for you to
consider and show your x-ray text so that if you’re looking to get that view
for your Ortho Potts and follow up, you can get the appropriate films. [00:53:00] Very little utility or time for the MRI is
gonna be useful. In the emergency department, we did highlight ultrasound and
its utility for bursal, bursitis, bursal disease, as well as tendinopathies
tendon ruptures to partial tears.
Uh, and then we started getting into our, our workup, our.
Outside of radiographs element, very little utility to serum blood tests. If we
are gonna be tapping a knee, which if we have any suspicion for septic
arthritis. Even if it’s he arthrosis versus we, we say let’s go forward with
it. Even on someone with anticoagulation, you’re data supported, obviously
you’re gonna be doing best practices to keep it sterile and try to avoid being
very traumatic and inducing a septic, uh, sorry, a he arthrosis, but very, very
uncommon And know that you can do this procedure safely without injuring your
patient further while you work ’em up for something more serious when you get
the fluid out.
One, there’s therapeutic value in that. Take as much of the
fluid out as you can in your, you know, osteoarthritic knee effusion to give
them some relief. Be [00:54:00] conscious and
cautious about the agents that you’re injecting into it. Ropivacaine seems to
be better than the other local anesthetics and sparing the cartilage.
Know that if you’re gonna be putting a steroid in, you’re
probably putting the person at least three months out from their total knee
replacement. So consider that, or at least have counsel with them about that
before doing that type of injection. And then when you pull your fluids, we’re
doing our cell count, we’re getting our differential of that cell count, gram
stain crystals and Lyme or other arthropathies vector-borne illness.
If you’re right in the right endemic area, how’d to do? Agreed.
You don’t need us anymore. Nah. Well, I’ll still have you interpret my
merchants use for me, but yeah. Dr. Parisian, I thank you so much for being on
the podcast. Very, uh, educational, entertaining, love having a familiar face,
and I learned a lot. I know our listeners did too, so thanks for coming on.
Robert Parisian: My
pleasure, Dr. Hine. Thanks for all you do.
Keeping your skills up in rare procedures is a battle you don’t have to fight alone. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off
Historical Insights and Identifying Repetitive Microtraumas
When dealing with any painful condition, history matters and this is no less-true for knee pain. Delving deep into patient history to understand the nature of knee pain can give very valuable insights and help clinch a diagnosis. Dr. Parisian emphasizes that knee pain often isn’t truly “atraumatic.” Instead, patients might experience repetitive microtraumas through certain activities, whether it’s extensive kneeling or sudden spikes in physical engagement like playing pickleball for prolonged periods.
Key Takeaways:
Always explore changes in the patient’s activity level to identify potential microtrauma.
Inquire about medication and social history, as factors like steroid use can affect tendon integrity.
The Comprehensive Physical Exam: Going Beyond the Surface
An essential part of managing knee pain is a thorough physical examination. Dr. Hine and Dr. Parisien discuss a systematic approach starting from neurovascular checks to assessing joint stability. They highlight the utility of specific maneuvers like the Lockman test for ACL integrity and McMurray’s test for meniscal injury. Being algorithmic can help you not miss anything: get them in shorts/visualize the knee. Feel it for warmth, check for skin breakdown, feel for effusion. Then work your way through an MSK exam. Starting with a straight leg raise lets you know their quad and Achilles are intact. Boom. Then move to slight flexion for Lachman (ACL, PCL), do a varus and valgus test (LCL and MCL respectively). You can then move into 90 deg flexion for an anterior-posterior drawer (ACL, PCL again). Testing points through a few different physical exam maneuvers can improve sensitivity of the exam. Dr. Parisien then also highlights the pivot shift test as his final ACL assessment. Finally, the McMurray test for the menisci.
While going through these tests and moving to various degrees of flexion-extension, palpable the anatomy to assess the alignment of the tibial plateau in relation to the femoral condyles
Key Takeaways:
-Begin with a straight leg raise to check for tendon ruptures and progress through various knee flexion angles.
-Doing several, quick tests of the same anatomical structure can increase testing sensitivity
-Understand the anatomy of the knee, focusing on how the tibial plateau aligns with the femoral condyles to identify misalignments.
Imaging and Diagnostic Steps: When to Use X-Rays
The discussion underscores the vital role of imaging in diagnosing knee issues. Despite some reluctance due to guidelines like Choosing Wisely, plain x-rays remain a crucial diagnostic tool, helping to identify osteolytic lesions, joint space narrowing, and even assessing hip alignment for comprehensive understanding.
Key Takeaways:
-Don’t hesitate to use x-rays in the diagnostic process; they can reveal essential information about knee and hip health.
-From an othropod’s perspective, the most useful views are the AP-lateral knee and the Merchant view (image below) to assess patellofemoral alignment accurately.
The Role of Ultrasound and Laboratory Testing
Ultrasound presents an effective, non-invasive method to enhance diagnostics, particularly for tendon evaluations. Meanwhile, serum labs often hold limited value unless specific systemic conditions are suspected. The conversation also details the utility and risks associated with joint aspiration for both diagnostic and therapeutic purposes. If you are worried about a septic knee, by all means tap the joint. Do not fear an anticoagulated patient for arthrocentesis to rule out septic arthritis. If the effusion is large and draining may offer significant relief, go ahead cautiously and be very aware of proper sterile technique.
Key Takeaways:
-Employ ultrasound to discern tendon ruptures and bursitis, making comparisons with the contralateral knee.
-Always do joint aspiration for cases with suspected septic arthritis, and recognize it is safe to do even in anticoagulated patients.
Management Essentials: Therapeutic Aspiration and Patient Counseling
Therapeutically, removing excess synovial fluid can offer significant relief in osteoarthritic patients. However, physicians should approach intra-articular injections with caution. If corticosteroids are injected, an orthopod may delay joint replacement for ~3 months because of increased risks with the surgical repair in the setting of these steroids in the joint. Removal of the fluid itself can have therapeutic benefits, and some ropivacaine (the least chondrotoxic local anesthetic) can be a good choice.
When conducting a joint aspiration, we are sending the fluid for several tests including cell count, differential, crystal analysis, gram stain, and culture to assess for conditions like septic arthritis. A synovial fluid white cell count over 50,000 cells/µL, especially with neutrophil predominance over 90%, significantly raises the suspicion for septic arthritis. In endemic areas, sending the fluid for vector borne illness testing should be considered, regardless of the time of year.
Key Takeaway:
When aspirating joints, ensure comprehensive fluid analysis is conducted to rule out serious conditions like septic arthritis, and counsel patients about the implications of corticosteroid injections on potential surgical timelines.
Conclusion
Overall, this podcast episode brings together practical insights and expert advice, equipping healthcare providers with a knowledge-rich framework to address atraumatic knee pain effectively in the ED setting. By integrating these evidence-based strategies, practitioners can enhance patient care and build a robust diagnostic regimen.