Hip Tricks: Battle of the Blocks
Contributors: Jason Hine MD
Welcome back to SimKit, and our podcast today on hip fracture blocks. Today’s post focuses on a significant study comparing peri capsular nerve group (PENG) block and fascia iliac block for managing acute pain in hip fracture patients. Conducted by D Pietro et al., this research, published in Anesthesia in December 2025, offers insights into pain relief techniques within a single-center academic site in Italy. The primary focus was on immediate pain relief achieved within 60 minutes of the block procedure, with secondary outcomes analyzing pain intensity and opioid consumption.
Transcript
+
Keeping your skills up in rare procedures is an uphill battle. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off
The Paper
Comparing the pericapsular nerve group block and fascia iliaca block for acute pain management in patients with hip fracture: a randomised clinical trial.This was by Di Pietro et al in Anaesthesia. 2025 Dec.[Pubmed]
Full citation: Di Pietro S, Maffeis R, Jannelli E, Mascia B, Resta F, De Silvestri A, Musella V, Centurioni CE, Regeni E, Grassi FA, Locatelli A, Perlini S; Regional Anaesthesia in Emergency Medicine (RAEM) Research Group. Comparing the pericapsular nerve group block and fascia iliaca block for acute pain management in patients with hip fracture: a randomised clinical trial. Anaesthesia. 2025 Dec;80(12):1484-1492. doi: 10.1111/anae.16695. Epub 2025 Jul 29. PMID: 40727959; PMCID: PMC12614414.
What They Did
This was a single Center academic site study in Italy comparing the pericapsular nerve block or Pang block to the fascia iliaca block for patients with hip fracture.
-Primary outcome was pain relief over a 60 minute interval after the block was performed
-Secondary outcomes included:
— The number of patients who had 33% and 50% decreases inThe SPID or summed pain intensity difference, on the visual analog scale (0 to 10 or 0 to 100 mm)
–The total amount of opioids administered in morph humility equivalents or MMEin the 60 minutes after the block
–Adverse Events
Patients were included if they were 18 years of age or older in the emergency department who had a radiologically and confirmed proximal femur fracture this could be subcapitate transcervical intro-canteric or paratrocanteric. they had to have moderate to severe acute pain with a score of four or 40 at rest or with movement, they had to have capacity to provide their own consent and be able to do the vas on their own.
patients were excluded if they had a known hypersensitivity to then aesthetic sub truck enteric diaphysical or periposetic fracture or hemodynamically unstable had a history of severe cognitive impairment or evidence of Dementia or delirium. they were also excluded if they had a BMI greater than 35 or were less than 40 kg
Study Design
Patients were randomized and then were tested for pain at rest and with movement which was hip flexion of 15° which seems like a terrible thing to do to a patient with a hip fracture but they had to get baseline scores. Patients were randomized in a one-to-one group to the PENG block or the fascia block. Smartly, when the procedure was performed the operating position who of course could not be blinded to what type of block was done they did used local disinfectant in both areas where the PENG block and the fascia iliaca block would be done.
The blocks were done by a total of six- initially four but two left the institution were replaced by two others- but a total of six senior Emergency Medicine physicians who are trained in both blocks. They were of course not blinded to the block technique but they completed the block and then we’re not in other ways involved in patient care so the treating Physicians and those assessing outcomes in pain scores were blinded to the block technique
interestingly all patients got 15 mg per kilogram of paracetamol or acetaminophen in the United States and none were to receive anxiolysis or opioids for the procedure block itself.
For the blocks themselves they used 0.375% Levobupivicaine and 4 mg of dexamethasone.For the pain block interestingly they got 20 ml of the Levo bupivacaine plus the decks and for the fascial block they got 30 MLS of the levobupivicaine + dex.
After the blocks were done patients had a Pain Scale assessment at 5, 15, 30 and 60 Minutes post block
They screamed 92 patients with 28 being excluded leaving 64, 32 in each group. interestingly and importantly there were two dropouts from the Pang block group. one because of body habitus precluding the ability to do the technique properly and one had a diaphysical fracture, so should have been excluded from randomization. with these patients they decided to have them have a percent SPID of zero in the intention to treat analysis. which actually shows potential signal for increased effect if they were included we’ll talk about that later.
Results
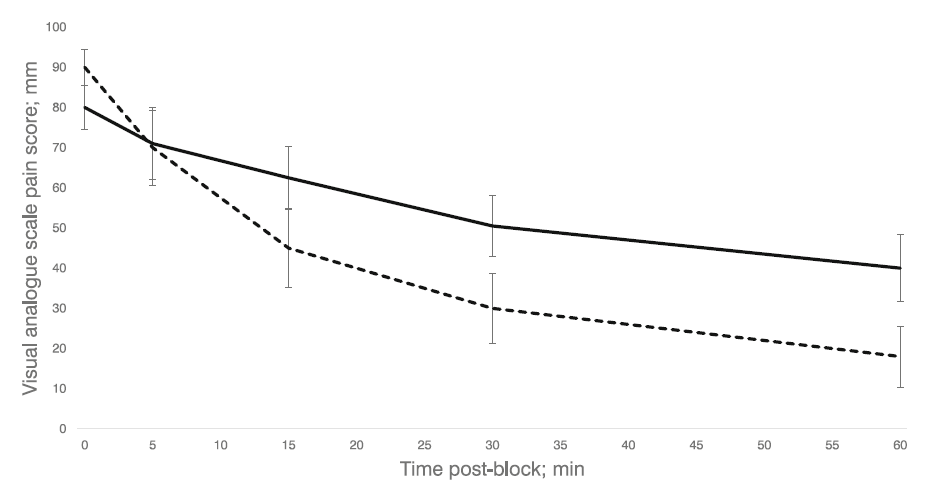
The PENG block group actually had a higher pre-block vas at average pains score of 90 versus 80. But the effects are pretty dramatic and are shown very well in Figure 2, reproduced below. By 5 minutes both groups had equal general pain at around 70 on the VAS, and from there the PENG block group dropped significantly relative to the facia iliaca block related to paint scores.
The PENG block group had a significantly greater summed pain intensity difference compared to that of the fascia iliaca block- 63% versus 38%.
33% SPID
Looking at how many patients had a 33% SPID change or greater we saw 28 of 32 in the PENG block group and 19 of 32 in the fascia iliaca block group
50% SPID
24 of the 32 in the PENG Block versus seven of the 32 in the fascia block. these differences were statistically significant.
For secondary outcomes, rescue analgesia was given in 5of 30 in the PENG block versus 10 of 30 in the fascia iliaca block group– different but not statistically significant. The average MME in the PENG block group was 3 versus 8 in the fascia iliaca block group.
Strengths
-This is a well executed academic study with generally good study protocols, blinding and follow-through.
-It is prospective data collection with independent observers minimized bias.
-While in academic center it is widely applicable to Emergency Medicine practitioners everywhere.
Limitations
-Details about the physician’s performing the block and their prior experience are limited.
-Exclusions of a BMI of 35 or higher is somewhat limiting particularly in the United States with the Obesity epidemic.
-They actually wanted this to be a two-site study but they were unable to enroll the second site so it is somewhat limited by being a single Center, but as noted in the strengths the topic and procedures performed are generally applicable and can be performed by most or many Emergency clinicians.
-They had the one patient excluded from the pain block group because of anatomy and one enrollment violation.
-They were underpowered for MME difference.
Discussion
The authors do a great job in their introduction of talking about multimodal analgesia and generally a desire for avoidance of significant opioids in frail elderly patients who tend to be those who break their hips. they cite the Royal College of emergency medicine best practice guideline about the use of the fascia iliac Block in the emergency department as a best practice for patients with this fracture pattern.
They present pretty convincing data though relatively small numbers with 30 to 32 patients in each arm about the improved efficacy of the paying block over the fascia iliaca. the authors also talk about the potential benefit, though less relevant for us Emergency Physicians, of the motor sparing of the quadricep with the Peng block.
The authors do a nice job of citing their own limitations which are similar to our own the idea of it being single-centered and ideally we would have loved to have that UK site involved, and the general short duration of observation of analgesic effect, stopping at 1 hour. I recognize why the authors did this to prevent confounding of physical exams by Consultants moving patients to hospital beds other things that are happening that might influence pain over time, but one hour of analgesia is good, but seeing the effect over a longer duration of time and the collective mme used by patients in the coming say 10 to 12 hours would be very insightful.
Authors' Conclusion
The PENG block provides superior analgesia for the first hour after intervention when compared with the infra-inguinal FIB and represents a promising modality for acute pain management in Emergency Departments.
Our Conclusions
I tend to agree. I don’t think that this is the most robust study we will have comparing Peng to fascia iliaca, but is a well conducted study and shows pretty dramatic effect related to pain scores and actually mme of opioids given. I personally don’t need a more robust study comparing these two approaches. cool I am in full agreement that a regional block should be standard practice for elderly patients with hip fractures. I myself have been a fascia iliaca block person for the entirety of my career, but recently have done a few of the paying blocks and with this study will have that as my first preferred location for elderly patients with hip fractures, keeping in mind body habitus, the fact that we are above the inguinal ligament and considering that related to anticoagulated state etc.- but when both are an option for patient I will be reaching for PENG.