Subscribe to the Podcast on



Podcast subscription form
"*" indicates required fields
Stroking Out in the Community
with Evie Marcolini
Contributor: Jason Hine, MD. and Evie Marcolini MD
Managing strokes in the modern era is challenging (lytics, EVT, timestamps!). Doing so in a community hospital, far from the ivory tower endovascular suite and neurology ICU can be even harder. We sat down with the very smart Dr. Evie Marcolini, EM and Neuro critical care doc, to talk managing these complex patients in these community settings.
Keeping your skills up in rare procedures is an uphill battle. The Sim Center or conference small group once a year (… or 2 years… or 5!) is not enough. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off
Transcript
Click below to see a full transcript of this podcast.
Transcript
Transcript
Jason Hine Hello. Hello. Hello. Hello, everybody, and welcome. Welcome back. Welcome back to the SimKit podcast. I am joined today by this is a special guest actually for me in Doctor Evie Marcolini. Evie has been a wonderful mentor for me throughout my career. As I developed myself as an educator, as a clinician. And you know, we’ve worked on many different topics and many different spaces together. If you look at the subarachnoid hemorrhage chapter of EMRap Core Pentium, you will see some familiar names included from this podcast. And she herself. She’s an inspiring educator in the space of emergency medicine and neurology, particularly in neurocritical care. And this makes her the ideal person to talk to today about our topic, which is the management of acute stroke in the Community emergency department. Evie, thank you so much for joining us. Tell the listeners a little bit about yourself and your experience, your practice environment.
Evie Marcolini Thank you, Jason. And I could not be more thrilled to be here. I’m so proud of you and what you have developed and it just it’s just so great to see everything that you keep building and and and all the great work you’re doing. So congratulations to you.
Jason Hine Thank you.
Evie Marcolini I tell people this all the time and it is from my heart. I have worked in a tertiary Medical Center my entire career. And I’ve always got resources. The folks who work in the hospitals without those resources, the community hospitals, the. Urgent care centers, the very rural hospitals are on the sharp end of the rope. They are the ones who are doing the hard work and I highly respect you all. And if I could do your job because I’m so used to having all the resources available, so my hats off to you all. I don’t. And my utmost respect for you, I. Finished emergency medicine residency at Maine Medical Center and I went on to do a surgical critical care fellowship at. Shock Trauma in Baltimore. Before we could board certify in critical care. After that, I stayed on as faculty at Shock, Trauma and University of Maryland for two years before moving back north and going to Yale, where I worked in surgical critical care emergency medicine, and then helped. Build a dedicated neurocritical care ICU. I stayed there for about 8 years and have moved on to Dartmouth where we have started a neurocritical care ICU in 2019 and I still continue to work a 5050 split emergency medicine and neurocritical care. And it’s a great split because I see the patients who come in the door in the emergency department, I see them go to the neuro. I see you and then onto the floor and it it’s a really good. Good. It’s a really good practice where I can not only understand. What happens coming through the door in the emergency department where we are the first ones to diagnose the patient and determine what happens in those really important first few minutes and the first hour. But then transitioning on to the ICU. And. It’s really helpful in my teaching because I have the perspective from both sides. I absolutely love neuro and neuro topics and emergency medicine, so I’m thrilled to be here talking. With you about it.
Jason Hine Thank you. Thank you again for joining us and thank you very much for your kind words. And yes, this is fantastic because as I mentioned this experience, you have, it really does make you the perfect person to talk to about stroke care in the emergency department. Now this stroke care has evolved significantly over the past 3-4 or five years. With the evolution of endovascular therapy. I kind of joke and I do sort of see like the neurologist. They have been searching for decades really to find an effective and active treatment for stroke. And we’ll talk about TPA or TNK in a moment. But it appears that we really have found one now granted, this is for a select minority of patients. Now, while this is great for patients and this disease process, it really has made management of stroke in the Community setting much more challenging and complex. So with that in mind, Evie, I want to talk about how you think community hospitals should be structured and how providers should be acting in these settings. How’s that sound to you?
Evie Marcolini Yeah, it’s really a. It’s really important to think about and let’s talk about that in 2015 before 2015. We didn’t have FDA approval of mechanical thrombectomy. We didn’t have evidence that showed that it improved outcome, but we were doing it all the time. There were so many patients who were having thrombectomy improving their outcome and having great outcomes from it. And it wasn’t until 2015, when we had the Mr. Clean trial that showed improved outcome and then the subsequent five other trials that corroborated that. They all close their books early because there was overwhelming evidence that mechanical thrombectomy improved outcome. Well, that’s great. And and it helped us to pursue that. But what it did is moved the needle because now when patients come into the emergency department. Not only do they have TPA, which we’ve argued and paddled for decades over, but now we’ve got something that really has great data behind it and that makes it so important to be acting quick.
And diagnosing and treating and getting the patients to the angio suite to improve outcome because time is still brain with thrombectomy just as it is with systemic thrombolysis. So that puts the onus on us in the emergency department wherever we are to understand what’s going on. To act quickly and to to get the patients where they need to. So if you’re in the community and you don’t have neurosurgeons that are doing endovascular thrombectomy. You’ve got to get them to that place. The other thing that has happened is it brings up the question, should we still be giving TPA? Should we still be giving systemic thrombolysis in the patients who are going to have mechanical thrombectomy? The short answer to that is yes, it still is the standard of care. To give patients systemic thrombolysis even as they’re on their way to mechanical thrombectomy, and we can, and we can talk more about that later if you want. But what this does is it pushes the decision making out to the pre hospital world. So folks who are picking patients up, diagnosing stroke and trying to figure out, do I go to the closest hospital or do I carry on to the tertiary care center where they can do mechanical thrombectomy it complicates the decision making. To be sure, and there are systems in the country. That have diversion protocols and and have worked together to figure out which patients should bypass the local hospital to get to thrombectomy. Not all systems have that and it’s really complicated and intensified the work that we do, both pre hospital. As well as in emergency departments to get these patients where they need to go.
Jason Hine Yeah. And I’m. I’m glad that. You brought up. That pre hospital because that is an additional wrinkle there. I mean there are so many decisions or decision points that need to be made as a provider that we’re going to get to in a moment that you have to do in moments, right? We have to score them on two different categories essentially and think about their likelihood of. Having an LVL large vessel occlusion as well as their candidacy for T&K TPA, so there’s a lot to do and there’s a lot of branch points and then as you mentioned those there are those that get both and so making that decision in the back of an ambulance with limited information makes that even more challenge. Now you can’t be diverting all patients with stroke like symptoms to your tertiary center. So there has to be a balance, right. There has to be balance in a mix there. But first, Evie, I kind of want to start with the brass tacks of stroke, the basics, the basic care, if you will. So that in mind, I want to paint a picture. I want to tell you about an 85 year old female. She comes in via EMS with dense left hemiparesis and garbled speech. The family noticed that Mima just didn’t seem right after breakfast. So. Naturally, they put her down for a brief nap. She woke up about two hours later and they noticed these deficits. So now we’re at the three and a half hour mark from last known well. Well, Evie, tell me about your approach to this patient with the pretense that you are now working in one of these freestanding emergency departments, but one that does have CT capability.
Evie Marcolini That’s a great case, so I know that I’m 3 1/2 hours out from last known well, so I’ve essentially I have an hour to work. With. Of the the systemic thrombolysis window. So the first thing I need to do are the basics of finger stick glucose, do an exam, get her to the scan. Those are the the three big things you know, to the scan to make sure she doesn’t have a bleed. And I I think it’s interesting in in this case where the family put her to bed. Because they said she didn’t seem right because that is. It’s pretty common that an 85 year old female might not seem right, and it might just be because she’s fatigued. She has a UTI. There’s so many other things that can mimic stroke. So it’s. Not really that unreasonable that the family put her to bed for a couple of hours. Thankfully, she comes in at the three and a half hour mark, but I’m trying to figure out does she have a bleed? If not by my exam, does she qualify for systemic thrombolysis? And getting that on board as soon as possible, even though we’re at the tail end of the four and a. Half hour window.
Jason Hine Yes, and and not to mention we have that sort of another hour to that 4.5 hour mark. But the second that they hit your door, you also have your own internal timers, if you will. You know your own systems based timers and we have 20 minutes to CAT scan. You know the time window for ourselves as an example. So you’re not only sort of competing against the clock of systemic thrombolysis, you’re also trying to work within the metrics within your system. So long as you’re doing, you know best by the patient, obviously you’re trying to meet these numbers as well. So there’s kind of two ticking clocks that you have to consider.
Evie Marcolini Yes, and and I will also add that you have to find out if this patient would want thrombolysis where it offered, if you could offer it, would she want it? She may not be able to tell you in this case, she’s not going to be able to tell you whether she would want it. You have to find out who her close. Family is who is her? A POA who is the person who’s going to be a surrogate decision maker for this now I’ll tell you, there are folks who argue that systemic thrombolysis is the standard of care, comma. Thus it doesn’t need consent. I am not one of those people.
Jason Hine Yeah, agree.
Evie Marcolini This is a procedure. This is a medication that has risk and it does need to be consented. It it is. If you cannot get consent then. Either by the patient or can’t find family members, then it’s reasonable to to give it because it is the standard of care. But we need to make every effort to present this as an option to patients and or their surrogate to obtain consent for it. So so you have to find the family and clarify when was the last known? Well, how did the story go? Because oftentimes the story changes when you actually get to the people who are. Right there with her.
Jason Hine Yep. Yeah. No, I totally agree. I think it’s it’s not without risks. And yeah, we actually we may possibly get into this later in the podcast, but I like being present during the consent process because. I think it’s nuanced and you know not to say that I don’t trust our neurologist to really outline them, but you don’t want the risk to be glossed over. You want to make sure the numbers are truly being presented in terms of bleed risk, mortality risk if bleed etcetera. Now in that space, Evi, just to go over this case a little bit more nuance in detail. We have a stroke stop in our department. You stop before you transition into the bed so you don’t have to turn this in the back out and all the delays and details that come with an EMS. Handoff, if you can tell me about what you’re doing at bedside or at stretcher side, in the hallway with this patient. Do you have specific scores that you’re referencing or doing and how are you coordinating that with the general approach with what you’re asking your nurses and? Techs to do.
Evie Marcolini Well, what we’re doing is getting a quick exam. We’re not doing a full NIH stroke scale. We’re doing a neuro exam to figure out, does the patient have a large vessel occlusion? Clearly, if they have stroke symptoms as this patient does, they’re going to get a CT. And they’re going to. We’re going to consider whether or not they they should be offered systemic thrombolysis. But it’s not the entire NIH stroke scale that we’re doing. We’re doing an abbreviated neurologic exam.
Jason Hine Perfect.
Evie Marcolini And that’s the first, and that’s the first step. I’ll tell you that there are some systems and I’m glad to hear that you guys have a stroke stop in the hall. Way some systems are going directly to CAT scan, getting the exam along the way and the finger stick getting an IV, and if it’s not already in and getting that CAT scan as soon as possible. Some systems are also pulling up the systemic thrombolysis whether it’s all to place because that alter place needs to be mixed right, and they’re pulling it up right away. And I think that’s great. It’s a time saver. And if it doesn’t get used, it can be replaced. It will be replaced by the company. That’s all time savers. When we think about stroke, we think about how can we shave off minus. Some systems are still not doing that. I will tell you that my system is not doing that. We take our patient to the room, we do the exam in the room, then we order the imaging and the patient goes off to the CAT scan after that and we’re not. Getting the TPA drawn up and mixed until we know we’re going to give it. There’s many reasons why some systems don’t do it that way, but I think that shaving those minutes is really helpful. So what you guys are doing is great.
Jason Hine Thank you. Yeah, I appreciate that feedback and every anytime you can save moments and it’s an you know it’s an aggregate of moments. It’s the opposite of death. By 1000 Paper Cups, it’s getting to your your numbers and metrics as as quickly and as efficiently as you. Can I’m gonna give you kind of my bedside approach and then I’ll ask for your feedback on it. How’s that sound?
Evie Marcolini Great.
Jason Hine So we often will and when our patients come through private vehicle, our numbers are worse 100%. We need to be better at recognizing stroke symptoms when private vehicle arrival. But we’re going to talk about the EMS. So in the EMS sort of alert via right radio, they will often tell us that they have a patient with stroke like symptoms. And that they are looking for a stroke assessment or stroke alert. With that in mind, we’ll often let our CAT scan know right away so that they can complete the last study and have the table held for the patient. When they come through the door, I’m working at bedside, I get the EMS rundown, particularly questions about last known. Well, if they’re on a thinner. Any other information related to trauma after that, while our nurses are trying to get our first set of vitals and our blood sugar, I’m doing our fast Ed assessment. I’m doing that scoring because our system works with that for differentiating concern for. Video and it is integrated in parts of it can be utilized in your NHS later on. So I like that system. I’m doing a fast D assessment, looking to see if we are at that four or greater point which we’re marking concerning for LVL. Once I get my fast Ed completed. I’m leaving patients. Stretcher. We are having a tech. Bring them to CT and I have to hop to the computer to put in the order for imaging, which includes generally a CT and CT Angio and you know the sort of laboratory work and and other things that go along with that. This includes a page out to our telestroke system. If we see a patient that we think is in the right window, a good candidate for TPA etcetera. After that order is in, I meet them in CT. CT is completed and I complete the remainder of my NHS at the bedside in the cat scanner. After that is done, the patients brought back to their room for the remainder of their sort of assessment, making sure that the labs are appropriately drawn. The persons on telemetry. We’re getting a cycle particularly important, obviously is the blood pressure so that we have that information for conversation with our neurologists from there, I’m usually getting a page. Back on my phone from our our stroke neurologist, we have the computer at bedside where we can do telestroke and we do the NHSS together and determine the appropriateness of we use TN. So that’s kind of it start to finish. What are your thoughts?
Evie Marcolini I love that I’ve I’ve I’ve taken some notes and I’ve got some some thoughts and also some questions for you. The stroke alert is is really helpful. I agree with you. It’s harder to do this. It’s harder to get the wheels moving when the patient comes in by private vehicle. We all suffer with that problem. And holding the CCT and getting all the wheels moving. Have do you page yourself or is there somebody who pages that when the stroke alert comes in?
Jason Hine We have a tech that calls our CT operator and lets them know we have a potential stroke for the hold.
Evie Marcolini That’s great. We do the similar thing when the stroke alert happens, a bunch of things happen all at once. What I think you have is an advantage, Jason is. When our stroke alert comes in in a tertiary care center, the stroke team comes down, but the emergency department team has started the exam and often there’s this little dance. Well, the Ed resident has started the exam with the attending standing there and then the stroke team comes down and the tendency is OK. Step aside. Let the stroke. Team do the exam and we’re we’re always trying to just get the the, the resident and the Ed team to continue that exam. And if there’s any questions the stroke neurologist can ask those questions and maybe. Finished parts of the exam that they hadn’t seen, so we we tend to waste a little time there. When you are it and you’re doing the exam and making the decisions, I think that’s a good streamline that you may not have been aware of really. You have an advantage there. And with respect to. Placing the orders, you’re doing that it it it’s similar. I think that’s the best you can do. You gotta figure out. What you’re going to get? Are you going to get CT or CT and CTA the fast Ed score is great. Whatever score you have in that your system uses and recognizes is the best one of the things about stroke care and keeping it streamlined and and not streamlined and efficient. Is doing the same thing every time and having everybody in the room understanding what’s going to happen. So so that everybody knows this. And when you you. You know this from from your company that teaches people how to get their muscle memory going by doing procedures stroke. The workup of stroke is the same thing. You’re it’s it’s muscle memory and it’s muscle memory for everybody in the room. And if 90% of the people in the room know what’s going to happen. Next it will happen and it will be efficient. So the fast Ed score is fine. Sometimes I talk about the van score from a study that by telling back in 2016, which is pretty simple and it it consists of asking how weak is the patient, can they raise? Both of their arm. Do they have aphasia or do they have neglect those three things? If they have weakness plus one or all of the those three things, they’re van positive and considered to be likely to have a large vessel occlusion, but it’s. Any system that you have that everybody understands is going to be the best system. And contraindications are a question as well. I have seen some systems that have different contraindications that are based in experiences that they have had. So there are the published contraindications and you could just you could just look at those on your MD. Milk, but the ones whatever contraindications your system uses, the the point of it is, understand what your system uses, know them, have them tacked up on the wall or in your pocket on a laminated card or something. Know what they are. Because that’s the standard that you’re going to be held to. And I say that. That and it sounds like I’m starting to talk a little bit about liability and I am because stroke is one of the highest liability cases in medical malpractice for emergency medicine. So we need to be aware of it and and when we talk about standard of care, we are held to the standard of care. That our hospital system uses. So contraindications are basic and they can be nuanced as per your hospital. And the the question of of CT versus CT and CTA is one that I’ve talked to a lot of people about. I I feel that getting a CTA. Is something that we should consider. It’s extra radiation. It’s extra cost. It’s contrast that an 85 year old person. Doesn’t have kidney problems yet may not really need and we need to be thoughtful about it. There are systems and folks that I’ve talked to. Who get CT CTA for every stroke and the way they justify that is that they say it’s not really a lot of contrast. It doesn’t usually box the kidneys and it’s very efficient on the side of efficiency. Those are folks in high volume places. I think if we’re in a place where we can take the time. To make the decision on whether or not we’re going to get that CTA, we should in our center, we do take the time to make that decision. It’s not everybody that gets a CTA along with their CAT scan. The other thing that I wanted to to bring up is, do you ever. Just give TPA without getting teleneuro involved.
Jason Hine That’s a great question. I would say generally, no, we have a robust enough system there where we have time by the time that we have our CT and our CTA completed, we have the ability to assess it. We have our full NIH score that we are in consultation with. Tell a neuro. Now, if there were a operation or system where that were down, there’s it problems technical issues where we can’t get the computer system to work. We probably default to a phone conversation, but in a hypothetical where we have no contact at all, say they’re already actively involved in the case and just can’t get themselves to our patient. We would be in the right to make that decision indeed.
Evie Marcolini Oh, that’s great. That’s really that’s really a great resource that you have. I I think that emergency medicine is really good at looking at the big picture. Neurology is really good at looking at the stroke picture. But one of the things that you may have seen this before are patients who come in.
Jason Hine Sure.
Evie Marcolini Looking like they have stroke, but what may have been overlooked is the fact that they have alcohol on board or there’s something else about their story that is a making this a mimic for stroke. Emergency medicine is really good at looking at the whole picture. And we all need to be thinking about mimics. Is this patient seizing? Is that a possibility? And getting the rest of the story from the family?
Jason Hine Yeah. Thank you for bringing that up and and also giving us that sort of liberty to be the bedside clinician and the clinician that generally can think with a broader scope, wider binoculars if you will, because yeah, you you may not like this, but I am not totally on board with systemic. Thrombolytics I do in very clear down the Pike, right down the fairway. Obvious stroke symptoms. Obvious time window. I I think it offers the patient the best opportunity for good neurogenesis. If there’s a wrinkles, complexities, other etiologies. If we’re thinking alcohol related. Or toss paralysis or anything else in that space. I’m often considering that talking about that, putting a time spent stamp in my note about why we need to further delineate the potential ideologies before giving this potentially harmful drug. So yes, I I agree wholeheartedly. And find it validating that you see us as the the folks that are best apt to really look at the whole picture and potential other ideologies.
Evie Marcolini Yeah, let’s talk about that. And I I you say I might not like it, but no, I completely respect that opinion that you just expressed. Jason. I really do. And I think that we are the ones that can help prevent giving TPA to stroke mimics and the other the other part of that is. Is that we’ve been arguing about TPA for decades, literally decades, and we continue to argue about it. One thing I I will say is if we’re not going to give TPA to a patient, it should be because we have a contraindication or the patient. Doesn’t want it after they’ve been explained what it is and what the risks and benefits are. And it’s always beneficial to bring a neurologist on board. Too many times, I see emergency physicians get in trouble when they make these decisions solo. And there can be consequences later that none of us wants to face. And this is the reality of our world. Even if we agree that the evidence for TPA improving outcome in somebody with a large vessel occlusion or even with a minor stroke is not great. The standard of care is such that we are held to it and I think we need to protect our patients by explaining to them really well what are the risks and benefits, but we need to protect ourselves by understanding what our hospital policies are and what we are expected to do. And and and hold to those. But if we’re, if we’re not going to give TPA, which I don’t support TPA in every case, we’re not going to give it, it’s got to be documented well and have a good reason. And it’s always a good idea to bring neurology on board with that decision.
Jason Hine Totally, completely, that that resonates super well with me. And if you, you know, look at the stuff by Mike blind stock or you look at. Any other things? That set you up for litigation, you know I. Don’t love to talk about that stuff because I. I think that is not our focus, right? We need to focus about quality care. But while we’re providing quality care, we also want to be able to practice for a long time and not be in the middle of a legal battle that can extend out for many, many years. So in that same space, as I mentioned, when we’re talking about and having those conversations and. There’s lack of clarity about Leo last known well. What if the patient actually? Had a fall. Or if they’re taking their anticoagulation all of these things are things that I’m time stamping, documenting in my note as to why, and in even in patients that. They don’t. It doesn’t suggest an LV or their imaging that firms is not an LVO, and they’re at that, you know, 4 1/2 hours say they’re at five hours. Still having the conversation with family like, I know that there is often talked about or you might have heard about clot Buster medicines, the reasons why we’re not using it in the circumstances, XY and Z and having that conversation. And having it documented I think is a hugely important factor in the care we provide just to protect ourselves.
Evie Marcolini I couldn’t agree more. That you you stated it quite. Well, thank you.
Jason Hine All right, so I wanted to come back a little bit to. We were talking about, you know, you can use the vans floor, you can use this SD score eventually you’re getting your NHS as they come back and go through that. Thank you for bringing back up anticoagulation or sorry, the the thrombolytic questions, right, we need to further delineate their candidacy. And the risks associated with it. So for our hospital system, we kind of have the, quote UN quote 3 thrombolytic questions. The 1st is, are they on an anticoagulant. And really here we are considering warfarin, dabigatran antenna inhibitors. And then any recent surgeries, trauma or major procedures, the definition of recently, I feel like that does evolve or will be variable by hospital system. So just make sure you’re aware of that where your system and where your autists are putting that number. And then any history of bleeding issues you know plug allopathy. And or major bleeds like an intracranial hemorrhage. So, I mean, what do you think about these questions as kind of goods or not good screening for thrombolytic candidacy?
Evie Marcolini I like those questions. I think that works quite well and the the other thing that that we’re doing in emergency medicine was we’re getting the patients history. We’re not just focusing on the the questions that. Would disqualify them for thrombolytics, but we’re getting their history to see if there’s any other nuanced things going on that make us feel that either a it’s a mimic or B it’s a contraindication. So if you go through a complete list of of of contraindications, getting a good history. Is going to pretty much cover all of those, right? Yeah. And you’ll find those things.
Jason Hine Yeah, true. OK, good, good advice. Get a full history. Talk to the patient at dying art in medicine. Probably just right behind an actual physical exam. All right, so every we’ve we’ve sort of talked a fair bit about our initial from the hallway structure assessment, the readiness of the system for rapid CT getting in touch with your knowledge. Some even of the medical legal aspects of talking about and consenting patients for thrombolysis. And then we talked about the true contraindications to thrombolytics with these questions. But there’s a wrinkle of complexity. For me that comes with the NIHSS. So I talked about the fast Ed and if the fast D. 4 is greater than four. That is an indication or a sign that the patient might have an LVL. But the NHS can also have a duality to it, if you will. So, as I mentioned, sometimes I’m looking for or trying to identify patients that may not really benefit from systemic thrombolysis. And one of the ones that’s in my mind is people that have low NIHSS typically talked about as a score. Under 4 obviously recognizing or considering the degree of disability from the deficits that they’re getting scored on. So lower NHSS might be a relative contraindication to TNK or TPA, but then there’s also the reality that the high NIHSS. So if you score someone and they have a score as six or greater as a potential trigger point for considering LVO, so kind of complicated. A difficult thing to work with. Evie, how do you rectify these kind of competing interests in the NIHSS?
Evie Marcolini So. I’m glad you brought up the NIH CSS and I’m going to take the liberty here of first talking about the NIHSS. I think we all know that this was a research tool developed. And it and it really evaluates patients for the anterior stroke and that’s the most common stroke. But I can’t resist taking the opportunity to talk about the fact that you can have an NIHSS 0. And have a posterior circulation stroke that is significant. So let’s not forget that we are putting more focus on the posterior circulation stroke now and I think it’s it’s bearing fruit because we’re starting to recognize that some patients who come in with dizziness actually have. Stroke. And when we’re talking about the cutoff points, when you talk about less than 4, less than six, greater than 6. I think we should be looking at what actually are the deficits. I can remember a patient that I had with an NHS of one who had isolated aphasia and. We gave her TPA and she got better so that she could speak. She was a young woman who would have been devastating if she couldn’t speak and so thinking about a score really doesn’t get specific enough in many cases. So if you’re saying to yourself I’m not going to offer. Thrombolysis because the score is low. That’s one of those times where I think you need to bring somebody on board. To help you support that decision because somebody could have off what what oftentimes gets referred to as a minor or non disabling stroke. That might be minor or non disabling to you or me, but maybe not to that person, so I’m not a big fan of seeing if a score is less than XYZ. We’re not going to offer. I think it has to be done on a case by case basis.
Jason Hine Yeah, I I like that approach and I think it it adds the simplicity and more of. A whole picture. Mindset like we’ve been talking about, which is really important, like you said, you can have low NHS and I’ve had those cases as well. As I mentioned, I’m I’m generally trying to find ways to wiggle myself out of going down that path. But people with a score of one or two who have profound dysarthria, or who have, you know, dominant. Weakness and their honestly, it doesn’t matter what your occupation is. If your dominant arm is no longer functioning, you’re still getting a relatively low score, but the deficit is pretty profound and devastating. To. You. So I like that idea of thinking about where the numbers are coming from. Where people are scoring in and I’ll tell you that. In my clinical practice, some people have had slightly higher scores. You know, I’m not pushing about four generally for this where there there’s a lack of clarity. There’s some inconsistent elements. The symptoms are largely sensory, with no pronator drift, no motor weakness. And those to me, I feel comfortable on my own. In some capacity, making the decision saying is a low NIHSS score. It’s related to a sensory change as opposed to motor or something that would be non disabling in that space and and for that reason we are you know the. Risk benefit profile for. And K is to not move forward so long as we’re completing a shared decision making with the patient or their proxy.
Evie Marcolini I agree and you bring up the sensory. If somebody has an isolated sensory exam, finding we have to think about. What you know you’re going to get imaging, but we have to think about, is this really a stroke and that that can become somewhat of a tricky question to to discern and those patients really are going to get neurology follow up they should.
Jason Hine Mm-hmm.
Evie Marcolini Because you don’t know, it could be it could be isolated sensory. So it’s it’s really good to bring them on board with that. And the other thing is sometimes I see people saying, oh, I’ve got this patient who’s got a right hand. Sensory deficit and. Right shoulder weakness and. Left arm sensory deficit and and you really. Need to put. That together and say, does this make sense anatomically? And if it doesn’t, then it’s probably not a stroke.
Jason Hine Totally agreed and I I forgot to put in my little Jabber joke about how there’s neurology data out there about about giving systemic thrombolysis to stroke mimics, and how it says, well, it’s not so bad because their bleeding risk is lower because they actually didn’t have a stroke. I don’t buy into that. I’m not drinking that kool-aid. Personally, I think we have to continue to. Think critically like, does this make sense in a brain and anatomic situation and and not just say, well, if I give systemic thrombolysis to a non stroke, their bleed risk is lower so I can go ahead and give it to everybody. But I I like this area of conversation about the nuances of the NHS and I’d like to kind of transition it slightly into this idea of dual antiplatelet therapy, because this is, you know, coming through in that 2023 article about lower stroke scores generally collectively not thought to be disabling. To the patient and having equipose, it seems in the treatment of uh, strokes with dual antiplatelet versus thrombolysis. So possibly another arrow in our quiver for these. Questions. And Evi, I just want to know, are you using this therapy and if so, how?
Evie Marcolini So. So, Jason, you’re talking about the ARAMUS trial from 2023 that looked at DAPT versus Alto place for patients with minor non disabling stroke within 4 1/2 hours from symptom onset in that trial that was defined as an NIH score of 0 to 5. With one point or less on single item scores such as vision language neglect or single limb weakness and a score of 0 and the consciousness item. So. If we go back to chance and point trials from 2013 and 2018, they showed US safety and efficacy with daft and acute minor stroke or Tia and the ARAMUS trial asks well why not Ulta place? And it was a multi center randomized open label blinded and point assessment non inferiority. Trial. They enrolled 700 patients and they showed that daft was non inferior with the primary outcome and excellent functional outcome of a modified ranking score of 0 to one. They also showed a secondary outcome that fewer patients in the DAP Group had early neurologic deterioration. They had fewer adverse events of symptomatic ICH and other bleeds. So with that study. It is a non inferiority trial. And and I’m no statistician, but I don’t think that that one trial shows that we should change practice and I don’t believe that the practice has changed, will it in the future change if we get some larger studies? And look at this and find out that daft is just as good as Alteplase for this probably.
Jason Hine OK.
Evie Marcolini And and I think my answer then to your question remains, it’s a non inferiority trial so. If you’re giving debt. Because you’re not giving TPA, I think the first the first decision point is, are we giving TPA and if if you decide with Telly, Neuro, we’re not giving TPA, then I think dapt is the standard of care.
Jason Hine OK. Yeah, I like that. I like that thought process and a branch point decision. And it’s a little bit different of an algorithm, I think for you than than the way that we’ve talked about or even used it in patients with these low scores, non disabling symptoms within a window for TNK. Or thrombolysis. We are sometimes talking about this as like do you do one or the other? I appreciate your branch point conversation, more of are we talking about systemic services, yes or no. And then if you’re in the no category, then you’re talking about utilizing dapt.
Evie Marcolini Yes. And also after that First branch point, if you decide we are not giving TPA because it’s non disabling or minor stroke. Then you are going to be getting an MRI and. Making a decision to give daft.
Jason Hine Yeah, that makes sense. And the the speed with which you operate for ADAPT is very different than that for T&K. So I appreciate that answer and that slight alteration and sort of mindset or or mind frame, the way you’re asking yourselves, those questions perfect. Thank you. Alright. So now heavy as we come. Toward the end, let’s talk about it. Let’s talk about the LVL realm. We’re gonna come back to MEMA Mema. We went to bed, came back wasn’t right. As dense hemiparesis on the left. Let’s say that patient upon your assessment, she has a fast Ed score of five. How does your approach differ when LDO is on the table saying we’re still in the window? Say she’s still coming in at 3. .5 hours.
Evie Marcolini Well, the everything we talked about with regard to the process of. Getting the patient to the scanner, determining that she doesn’t have a bleed and getting finger stick glucose in the exam, etcetera, applies. But if she if she, if I think she has an LBO, I’m going to get CTA. I’m also going to make sure which I believe we’ve already covered that. Somebody. ‘S calling. To see if we can get them to a center that has. Thrombectomy capability. The other thing, and I’ve heard some systems talk about this, is as you know. When EMS brings the patient in. And you’re doing everything that you do if they leave. And then you determine you want to ship your patient 45 minutes up the road. You you need to get another EMS rig to come and transport your patient. If you think there’s an LVO and you have the opportunity to ask EMS to stay, because then they can just take the patient right up the road to the endovascular center. That’s going to save time. That’s going to be very efficient. But I think where you’re going is when I know that the patient has a score that says probably in LVO I’m going to do everything with the anticipation of transporting to that center.
Jason Hine Perfect. I like that structure and that thought process and it’s another opportunity for listeners to think about their systems based practice, right. If you have a transport team that’s bringing a patient in and they are, they’re doing handoff, you’re doing your fast D score or your van score recognizing high probability for LVL. You’re going to scanner. You’re getting your CT probably. ETA. You’re getting ready and administering thrombolysis. That is not a long period of time, and having them available to complete transport to get to EVT is a great way to have that system in place. You do have to make sure that your EMS directors are on board with that process, but a huge time saver. For transport up to. ET and we definitely hashed this out, but just to say it allowed further, you are still, you know, I know there’s data about and conversations about if someone’s getting EVT, do they need systemic thrombolysis you’re still thinking with the same cap rate if you’re in that four and a half hour window and you’ve done all the things that you are supposed to do as a practitioner. You’re confirming that this is indeed a within the window stroke you’re giving your systemic thrombolysis as you prepare for the next step to the patient, which is EVT.
Evie Marcolini Exactly.
Jason Hine Excellent. Now let’s talk as a wrap up about how. You manage these patients say Mima comes in at six hours. So how do you approach her if she’s no longer in a systemic thrombolysis candidacy realm. What you do? Your VAN or your FAST ED and you have a high concern for LVO.
Evie Marcolini Yeah. And and I I I have pre hospital roots. So I always like to go back to the pre hospital and a question like this if the pre hospital team suspects that there’s LVO and they know that they’re past the four and a half hour window. There has to be some kind. There should be or it would be great if there was some kind of a systemic support to, say, bypass the local hospital and go directly to the the tertiary care center, where you can get thrombectomy. I think that’s not the case in most systems. I don’t know if it’s the case in your system. But that’s a huge time saver if if they can do that. And clearly, when we’re at six hours, we are out of the window without question for systemic thrombolysis and we would apply all of the. Imaging exam history, etcetera that we’re doing to figure out if we think this patient is having a stroke, we’re doing all the same things, but we’re focusing on getting them to a place where they can have the opportunity for thrombectomy.
Jason Hine Perfect. I love that. I like that process. I we talked in the beginning about how. You can’t be sending all of your stroke patients to the tertiary center. They’re going to be inundated and get poor care because of the number of patients they’re trying to deal with concurrently. But these patients outside of a window where you were intervention of TNK or TPI is really is not on the table any longer, but they just need to get to the place. Where EDT can be done and the EMS personnel are appropriately trained and able to do advanced or fast fees for other assessment for high probability L. You know, having those patients bypass is a fantastic idea.
Evie Marcolini Yeah. I I just want to say that. Stroke is a team sport. It takes, it takes everybody being on board with how to do it best. That’s pre hospital, it’s emergency medicine that includes nursing, tax, transport, physicians, everybody. And also system wide with hospitals that are sending hospitals, hospitals that are receiving hospitals, it’s really helpful to do Qi. It’s really helpful to look at the cases that you’ve had over the past month or two or three months do it quarterly do it monthly. And learn from each case. Stroke can be very complicated. Each case is very different. It’s really nice if you can have your endovascular neurosurgeons come and do some Qi and look at each case and and see what happened to them. See how they did. What happened with the patient? Did they do thrombectomy? Was it successful and and have that that, that whole team everybody’s in on it, this is a really complicated area. The the, THE imaging and the studies looking at how far we can push the window are are happening so quickly and I think it’s challenging for emergency medicine to stay on top of all the studies and everything that’s happening in the world of stroke because we’re also. Needing to stay on top. Of the studies and everything that’s happening in cardiology, respiratory and everything else. So it’s really it’s, it’s helpful to have that team approach to it and to embrace Qi and to say, hey, come down, look at our cases and go over them with us, I think. If I can say from the tertiary care center perspective, we often see some things that we say ohh this could have been better, but we don’t have the window. To approach that, because many times it would be perceived as the big dog coming down and telling us what we did wrong, but that’s not really what we want to do. What we want to do is just make patient care better. And I think if there’s a 2 pronged giving and receiving. Of quality improvement information we can make this better and we can learn in the process. I am always learning from my stroke neurologists every single day and it’s always a conversation. And so I I would encourage. Folks who are listening to this, if you’re part of a system where you don’t have that resource in house, look for Qi. Ask for it.
Jason Hine Completely agree. I think you know that comes back to as we talked about briefly, the idea of what we think it is about and and preparing right preparing for these are not actually that uncommon that infrequent. But if we don’t have the systems in place, don’t have a mental model and a shared mental model with our tertiary center, we’re going to set ourselves up for delays. And this is and this administrations. And all the above. So Evie, if I may, I’m going to do a summary and have you weigh in at the end. How’s that sound?
Evie Marcolini Sounds. Great.
Jason Hine Awesome. All right, so we were joined obviously by Evie Marcolini an Ed Physician as well as a neurocritical care doc to talk about stroke and the management of it in the Community setting. A fair bit of our conversation actually surrounds system based practices and best practices. The example that I gave was an elderly lady who came in at 3 1/2 hours and how we manage her in the Community Hospital or the free standing Ed. Ideally we’re getting a system in place where our EMS personnel can alert us so that we can be ready. We need to be ready as providers with our charge nurse, our techs and CT tech. If you can have a system where they do a stroke stop or giving report, someone is calling to hold the CT scanner so that you can do your initial assessment. You’re going to do a modified version of a neuro exam. And really in my mind, a lot of this is focusing focusing on the realm of LVL. He uses the van score. I use the fast DD score. Whichever your system has adopted, making sure that you’re ready and able to do that at bedside. When you complete that exam and you see signs for a stroke and you’re verifying that we are within a window, then you’re doing your processes or putting them in place to get the imaging order that you need and the additional generally should be order set based process for things like the blood sugar, the cereal vital signs, the EKG. Etcetera. I love the idea of working with our EMS personnel who both alert us of the patient coming in and if they are seen signings for an LVL, having them on standby for transport after we do our CAT scan, if they receive their thrombolytics, etcetera, they go up for EVT. We then started to get a little bit into the nuances of the NIH s s and how we think about numbers and patients, and I really like the global idea of it’s the patient’s, their history and what their deficits are and what they mean to them. When we make a decision about thrombolysis or not. Not necessarily considering a true number on the NHSS, but how devastating are the symptoms and how likely in the global picture of the patient their past medical history, the cancellation information we gained from the Ms. and family about what we’re actually dealing with? Are we confident that we’re dealing with a stroke or is there a higher probability of an alternative diagnosis with that documenting our thought processes in real time to protect ourselves medical legally, we’re asking our thrombolytic questions. We have 3 in our system, but making sure again reiterating the idea of working with our tertiary center for the questions that we want to ask to make sure that this patient is indeed safe for TNK or TPA. After that administration is done, and if we see an LVO, we are hopefully getting them back on the same EMS rig up to the tertiary center. If not, we’re working on trying to get rapid transport to these patients to the facility that’s going to care for them best in the long term. How’s that sound?
Evie Marcolini I mean, you have summed it up really nicely and hit all the high points that I think are really important when we’re thinking about stroke outside of the tertiary care center. The two things I wanted to add are #1 don’t forget about the posterior circulation. Book. Think about the dizzy patient. Understand the hints exam. Understand that a posterior circulation stroke will be treated the same as an anterior circulation stroke with regard to systemic thrombolysis and and sometimes will warrant thrombectomy. Many of them are also dissection and we need to find those. Those are can’t misdiagnosis. And the last thing I wanted to say. Is I’ve had. So many questions and conversations with folks about TPA and I’m not, I’m not one who argues the data and argues. The validity of the data, because I’m really not a statistician. But I do want to say that this becomes an ethics issue for me. And when I think about TPA, I really don’t think about giving it. I think about offering it. And we should be offering this to our patients and that means we need to be consenting them for it. And what that means is we need to be able to explain stroke in an understandable way to our patients so that they truly understand the risks of TPA. And the benefits of it and the risks of not taking TPA and the benefits of that, that it is the art that I think in emergency medicine we are very good at, we are very. Good at approaching a patient and getting to know them as much as we need to in the 1st 5 minutes so that we can figure out what do they understand? What can they understand and how can I explain the risks and benefits to them? We are really good at that. Because that’s what we do all day, every day. The other part of it is is understanding how to figure out what their risk taking propensity is. Everybody’s risk taking. Propensity is different. Yours might be different from mine. And we need to respect that, but we understand how to talk to patients and get at that. We do it every day. And I think if we approach the question of systemic thrombolysis from the perspective of we should be offering TPA to patients, it really does put a. Different feel to it. Then we should be giving patients TPA.
Jason Hine Yeah, I love that structure and that sort of mindset of offering it. And and we’re not going to get into the can of worms about TPA, TNK, collectively, as we wrap up. But I think if you were understanding of the literature and and hopefully if you’re forming a strong opinion you’ve you’ve read it in, you’re doing an informed consent. With that in mind, then you’re doing best by the patient, right? You can talk to them honestly or earnestly about how you about the data that’s out there and we’re doing that in concert. Of course, we learn our ologist if we’re going to have that conversation and certainly for giving these lyrics. Then we are going to be working with them very closely, but if you are informing them you’re doing that with your full spectrum of knowledge and that I think addresses this relatively sticky issue, but the idea of offering over giving of consenting rather than just treating without. Full understanding of their disease processes and their risks and benefit. I really love that approach. So thank you, Abby.
Evie Marcolini Thanks for having me.
Jason Hine Yeah, it’s been a blast. We will have you on again and everybody listening. Thanks for joining us today and I hope that we’ve helped informed your care of patients who present to your remote access freestanding or other Community Hospital with signs and symptoms of stroke until next time.
Overview
Managing acute stroke symptoms in the Emergency Department requires significant forethought, planning, and team coordination.
These patients have several time constraints that need to be navigated:
- Consideration for thrombolytics (TNK or TPA): Literature and best practices often put these cut points as 4.5 hours from onset of symptoms.
- Consideration for endovascular therapy (EVT): At the time of this writing, most literature and hospital systems support a cut point of 24 hours from onset of symptoms for patients with a large vessel occlusion (LVO).
- System level cut points: Like it or not, many hospital systems has quality metrics in place for patients with signs and symptoms of acute stroke. These can include time to EKG, time to fingerstick glucose, time to CT, time to neuro consult, and time to thrombolytics… just to name a few.
With the number of time-sensitive steps necessary to provide quality care of an acute stroke patient, the work of the EM physician and EM team can be daunting. Preparedness and practice is the name of the game.
The Approach
The Alert
Being prepared to receive a patient with acute stroke symptoms is the first step in the care of these patients. Having an EMS reporting system that relays key information (vital signs, last known well, etc.) in a succinct fashion in integral to success.
For walk-in/ from the waiting room patients, care can often be delayed and many systems struggle with meeting metrics for stroke patients from the WR. Triage nurse education and an alerting system can help improve performance here.
Rapid Assessment
Once the patient with acute stroke like symptoms has been identified, finding the space to assess them, ask pertinent questions, and examine them is the next challenge.
Having a designated area like the “Stroke Stop stretcher” outlined by Dr. Hine can help keep this from being a scramble. Being in close proximity to the ambulance bay and assessible from Triage are important consideration.
Once the patient is in a space to allow the team to assess them, many things have to happen either in parallel or rapid succession. These include:
– Patient registration
– An EKG
-A point of care glucose
-Vital signs
-Pertinent history (last known well, medications including anticoagulants, etc).
-A basic neuro exam*
-IV access
Some of these elements have competing interest and team coordination is vital. For example, patient history can coincide with the IV and POC glucose. The EKG and basic neuro exam cannot, so letting the team members know the order and sequence of events as the provider is important.
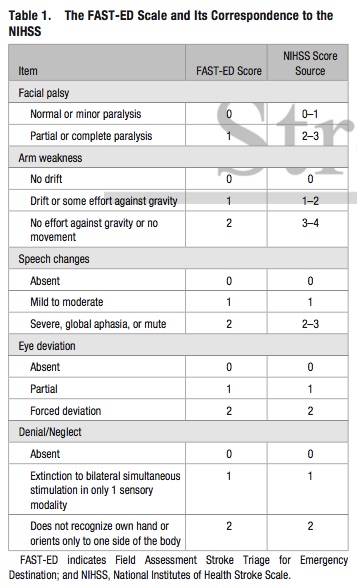
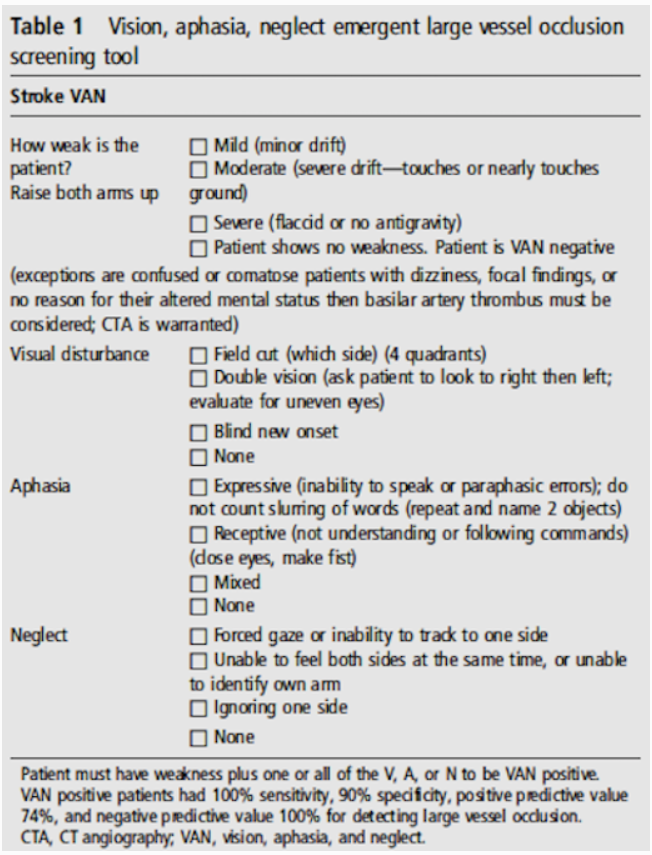
*With regard to the neuro exam, Dr. Marcolini agrees with Dr. Hine that a full NIH Stroke Scale (NIHSS) is not vital in this initial phase. There are several stroke screening exams. Dr. Hine uses the FAST ED score and Dr. Marcolini recommends the VAN score (see images below). In his health system, Dr. Hine notes a FAST ED score >4 is a marker to consider LVO.
During this initial assessment, it is important to consider the patient’s contraindications to thrombolytics. These can include any variation of the following, and should be agreed upon by your local neurologists:
- Is the patient on any anticoagulants? (warfarin, dabigatran, Xa inhibitor)?
- If so, when was the last dose?
- Has the patient had any recent surgeries, trauma or major procedures? Definitions here on “recent” and “major” are important to outline ahead of time.
- Does the patient have any history of bleeding issues or known coagulopathy and or major bleeds like an intracranial hemorrhage?
Imaging and Consult
After the initial assessment, the patient needs to rapidly go to imaging. This is to rule out an intracranial hemorrhage and, depending on protocol, assess for findings of large vessel occlusion.
Getting the patient to the CT scanner promptly is important and the topic of many hospitals’ metrics. For example, Dr. Hine’s institution has a 20 min to CT metric. To ensure speed and efficiency, processes can be put in place such as alerting the CT tech of a potential stroke patient upon EMS alert or initial assessment and holding the table for their immediate arrival.
While the patient is getting their CT, the provider can pursue a full NIHSS and consult neurology.
The Next Steps
After neurology is consulted and the patient is back from their scan, it is important to do a reassessment of symptoms as rapidly improving symptoms may affect the thrombolytics decision.
Thrombolytics Decision
The decision on whether or not to push thrombolytics is not a trivial one. This post is not here to dive into the strengths and limitations of the thrombolytics data (Dr. Hine and Dr. Marcolini may have slightly different perspectives on the validity of the data, have a listen!).
Whether or not you believe in thrombolytics, we all have to recognize that TNK/TPA is considered the standard of care in acute stroke patients within the window and without contraindications. Dr. Marcolini has a wonderful perspective in this medicolegally challenging place in medicine:
All patients with acute stroke symptoms within the thrombolytic window and without contraindications should be offered thrombolysis.
This is a very reasonable recommendation and carries with it the importance of informed consent. Dr. Marcolini makes the clear statement that a patient or surrogate decision maker needs to be educated on the medication, its potential benefits and potential harms before administration.
Steps from Here
Whether or not your patient gets thrombolytics, dual-antiplatelet therapy (DAPT), goes onto EVT, or has no such intervention, they often require further care and hospitalization.
Where this care is provided will depend on your practice environment and relationship with your neurology colleagues.
Take Homes
The patient with acute stroke like symptoms requires a well coordinated Emergency Medicine team and healthcare system prepared to assess these patients rapidly.
The following steps, done in preparation for these patients, can help facilitate timely and quality care:
- Having an EMS alert system with pertinent data
- Triage nurse education on the signs and symptoms of stroke and the system’s processes for assessing these patients
- A means of alerting providers of patients with acute stroke symptoms
- A designated (though not necessarily single purpose) space for the team to preform the initial assessment
- A coordinated, team approach to gaining history, access, EKG, POC glucose, vital signs, and focused physical exam
- A means of alerting the CT scanner of a potential stroke patient so the table can be held
- A rapid consult system with your local neurologist.
References
- Warner JJ, Harrington RA, Sacco RL, Elkind MSV. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke. Stroke. 2019 Dec;50(12):3331-3332. doi: 10.1161/STROKEAHA.119.027708. [pubmed]
- Hurford R, Sekhar A, Hughes TAT, Muir KW. Diagnosis and management of acute ischaemic stroke. Pract Neurol. 2020 Aug;20(4):304-316. doi: 10.1136/practneurol-2020-002557. [pubmed]