Piece of Cake: DKA/HHS Update Part II
Contributor: Dillon Warr, MD and Jason Hine, MD
Guest:�George Willis, MD, FACEP
Welcome to our Part II of our talk with Dr. George Willis, the endocrine expert, on��Diabetic Ketoacidosis (DKA)�andHyperosmolar Hyperglycemia State (HHS). In it we review The American Diabetes Association consensus report.�In Part I, we discussed epidemiology, pathophysiology, and clinical presentation of DKA/HHS.�Check out Part 1HERE. �
In Part II, we continue our deep dive into with a focus ondiagnostic criteria updates andnew
treatment guidelines. We break down the latest consensus statement and
discuss how these changes impact clinical practice.
�
Keeping your skills up in rare procedures is an uphill battle. Let SimKit do all the heavy lifting with simulation training that delivers to your door once a month. Use coupon code SimKit10 for 10% off
Key Points
- The diagnostic criteria for DKA have changed, with lower glucose cutoffs and beta-hydroxybutyrate as the preferred ketone marker.
- Fluids matter! Balanced solutions like LR and Plasma-Lyte are now first-line choices.
- Subcutaneous insulin protocols (SQUID protocol) are the new hotness inDKA management and can reduce ICU admissions.
- Early basal insulin can improve transitions off IV insulin.
- Electrolyte management, especially potassium, remains critical in avoiding complications.
Diagnosis
Diagnostic Criteria Updates
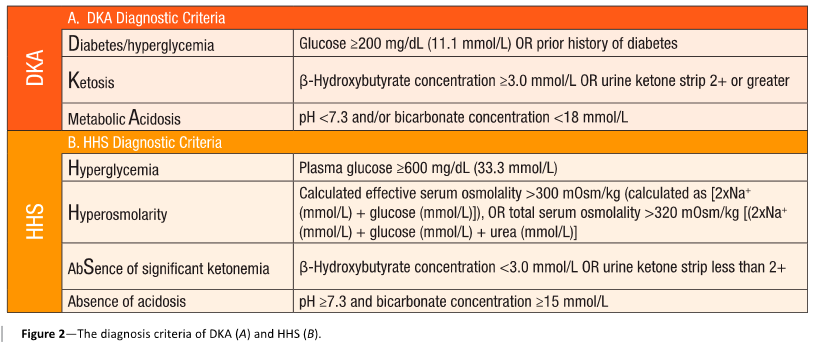
- The glucose threshold for DKA diagnosis lowered from 250 mg/dL to 200 mg/dL
- Recognition of euglycemic DKA in patients with low glucose levels but meeting other criteria
- Beta-hydroxybutyrate included in the diagnostic workup as the preferred ketone body marker
- For the acidosis, the criteria are pH < 7.3 or bicarb < 18
- Serum osmolarity calculations now a recognized tool for diagnosing Hyperosmolar Hyperglycemic State (HHS)
- The concensus statement has a great graphic reproduced below that should be added to your peripheral brain (smart phone) for quick reference:
Lab Testing & Initial Workup
- Standard lab panel includes glucose, electrolytes, anion gap, beta-hydroxybutyrate, and VBG.
- End-tidal CO2 > 27 mmHg may help rule out DKA quickly
- Importance of differentiating DKA from HHS based on sodium, pH, bicarbonate, and ketones
Treatment
Fluid Resuscitation
- Balanced crystalloids (LR, Plasma-Lyte) now recommended over normal saline
- Adjustments for patients at risk of fluid overload (CHF, renal failure)
Insulin Therapy
- Bolus insulin no longer recommendedbefore starting an insulin infusion. This practice has been common but is now census supported.
- For HHS, 0.05 u/kg/hr is a great start. For DKA, it is 0.1 u/kg/hr�as a standard start.
- New option for subcutaneous insulin in mild-moderate DKA using the SQUID protocol
- Early initiation of basal insulin to improve transition off IV insulin
Potassium Management
New potassium replacement guidelines:
- >5.0 mEq/L: Start insulin without supplementation
- 3.5–5.0 mEq/L: Start insulin + potassium replacement
- <3.5 mEq/L: Delay insulin, aggressively replace potassium
Other Electrolytes and Considerations
- Phosphorus supplementation only if symptomatic
- Allowing patients to eat during treatment if tolerated
- The major risks to these patients in treatment are hypoglycemia and hypokalemia. Beware this issues and allow the patient to eat for repletions.
- For pediatric patients, beware cerebral edema
- HHS is a slow process to happen and should be a slow one to fix. They all should be admitted to the ICU.
References
Umpierrez GE, Davis GM, ElSayed NA, et al. Hyperglycaemic crises in adults with diabetes: a consensus report. Diabetologia. 2024;67(8):1455-1479. [pubmed]
Griffey RT, Schneider RM, Girardi M, Yeary J, McCammon C, Frawley L, Ancona R, Cruz-Bravo P. The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. Acad Emerg Med. 2023 Aug;30(8):800-808. doi: 10.1111/acem.14685. Epub 2023 Feb 27. PMID: 36775281. [pubmed]
Hunter C, Putman M, Foster J, Souers A, Rodriguez A, Zuver C, Papa L. Utilizing End-Tidal Carbon Dioxide to Diagnose Diabetic Ketoacidosis in Prehospital Patients with Hyperglycemia. Prehosp Disaster Med. 2020 Jun;35(3):281-284. [pubmed]
�
Subscribe to the Podcast on


