PENG Nerve Block
Overview
The PENG block is an alternative, effective method to provide pain relief following trauma or analgesia before /after surgery to the hip and pelvis. It can be especially useful in elderly patients, who have a higher incidence of hip fractures and are more prone to adverse effects of IV anesthesia (i.e. opioids). The PENG block is a relatively new block, first proposed in 2018 as an alternative to the fascia iliaca compartment block. In contrast to the FIB, the PENG block is a motor-sparing block with target nerves being articular, sensory nerve fibers. When performed well, significant pain relief will be achieved while preserving a neurologic exam.
Indications
Analgesia for hip and pelvis injury. Please consider performing this block in patients with proximal hip fractures (above the level of the trochanters) and for pubic rami and acetabular fractures.
Contraindications
There are few true contraindications to this block. They include:
- Infection (cellulitis) at the site of injection
- Allergy to local anesthetic being used
- Patient refusal or patient who is altered and not able to consent to the procedure.
- High velocity trauma patient at high risk for compartment syndrome should not have this nerve block performed
Some relative contraindications to conside
- Patient needs a neural exam of the affected extremity
- High risk of bleeding or bleeding disorder particularly thrombocytopenia with platelet count <20. Anticoagulation is not an absolute contra-indication to performing this block.
- Prior neural lesion or active injury
- Previous femoral vascular graft surgery
Anatomy
The articular nerve fibers are accessible at the inguinal crease (below the inguinal ligament and intraperitoneal space), between the anterior inferior iliac spine (AIIS) and the junction of the ilium and pubis, known as the iliopubic eminence (IPE). The femoral head is easily identified initially. By sliding your ultrasound probe superiorly, the AIIS will be located as the ‘trough’ created by the pelvic bone. The psoas tendon, femoral artery and nerve are also easily visualized in this one view. Once this area is identified, it is targeted by a regional block that instills local anesthetic into this area. This block is safe when appropriate landmarks are identified because (1) there is a ‘bony block’ of the pelvic bone that acts as a backstop to the needle and (2) the block is performed relatively safe distance from the femoral artery, vein and nerve.

See the boney ‘trough’ that serves as the target of needle. Superior to this trough lies the psoas tendon. This is the target point, around which you will instill your local anesthetic.
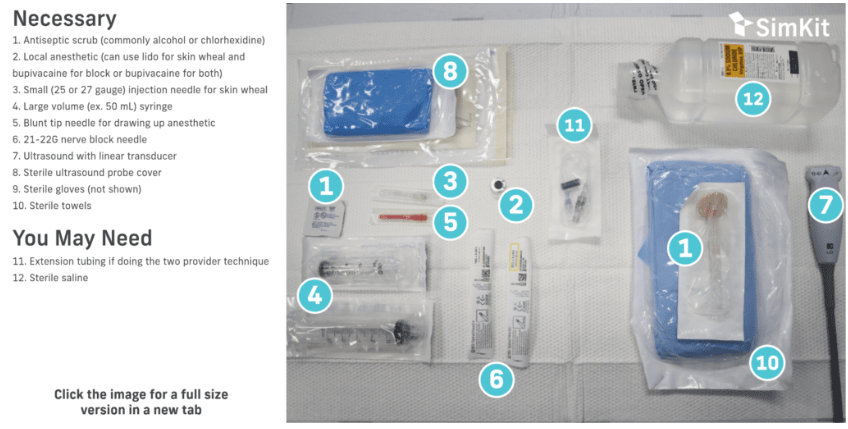
Materials
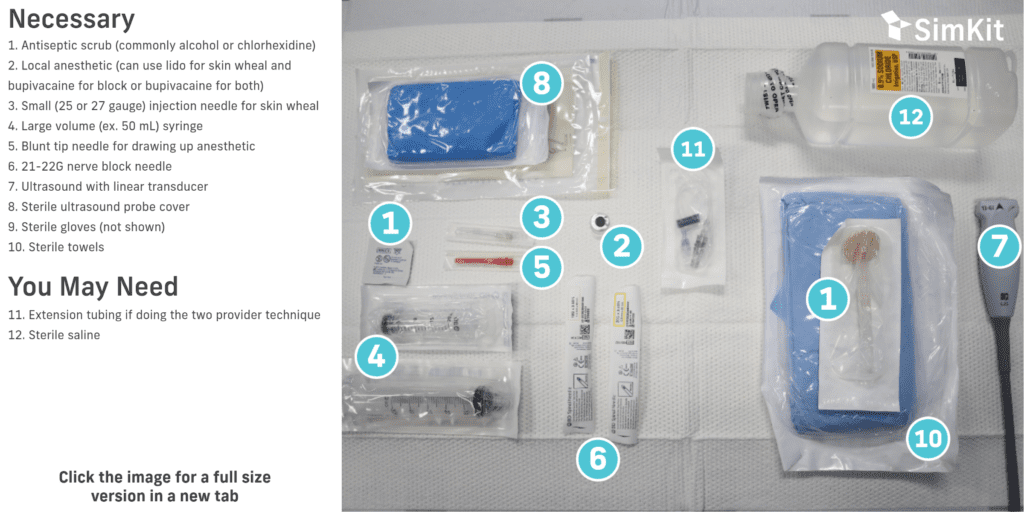
Note: Bupivacaine or ropivacaine are local anesthetics of choice given their longer duration of action. Bupivacaine has a maximum dose of ~2.5 mg/kg. The PENG block is a high volume block although less volume required (15-20 ml rather than 30ml for FIB).
Consider LAST treatment location in your department and monitor for signs of development. Always calculate safe anesthetic dose based on patient weight and concentration of medication.
Technique
Blocks should be performed with aseptic technique using a skin antiseptic, sterile field, and sterile equipment if possible. Allow for appropriate dry time for your antiseptic. Block needles should be aspirated prior to every injection to avoid intravascular administration, and injection should be immediately stopped if the patient suddenly complains of pain or high pressure.
Procedure with step by step process:
- Place patient in supine position.
- Clean the area with antiseptic solution and drape the area with sterile towels (image 3).
- Find femoral head with probe in transverse position
- Move probe superiorly and located AIIS and femoral artery/ vein
- Rotate the probe into a slightly more ‘diagonal’ position that is parallel with the inguinal crease
- Identify the landmark “trough” of bone medial to the AIIS and PSOAS tendon. Femoral artery and nerve should be in view to prevent accidental vascular or nerve injury.
- Place a skin wheal at injection site.
- Introduce the needle lateral to medial in-plane to the probe and advance the needle steeply into the trough, just lateral to the psoas tendon
- After aspiration, inject anesthetic to visualize lifting of the psoas tendon off the bone and a plane of anesthetic just above the pelvic bone. If resistance is met at this step, try twisting your needle tip. If continued resistance is met, withdraw needle slightly
- Continue to inject 15-20cc of anesthetic.


Summary & Bullet Points
PENG Nerve Block
Overview

Indications
Analgesia for hip and pelvis injury. Please consider performing this block in patients with proximal hip fractures (above the level of the trochanters) and for pubic rami and acetabular fractures.
Contraindications
There are few true contraindications to this block. They include:
- Infection (cellulitis) at the site of injection
- Allergy to local anesthetic being used
- Patient refusal or patient who is altered and not able to consent to the procedure.
- High velocity trauma patient at high risk for compartment syndrome should not have this nerve block performed
Contraindications
Some relative contraindications to consider:
- Patient needs a neural exam of the affected extremity
- High risk of bleeding or bleeding disorder particularly thrombocytopenia with platelet count
- Prior neural lesion or active injury
- Previous femoral vascular graft surgery
Anatomy

Materials
Technique
Ultrasound
Place patient in supine position.
Clean the area with antiseptic solution and drape the area with sterile towels (image 3).
Find femoral head with probe in transverse position
Move probe superiorly and located AIIS and femoral artery/ vein
Rotate the probe into a slightly more ‘diagonal’ position that is parallel with the inguinal crease
Identify the landmark “trough” of bone medial to the AIIS and PSOAS tendon. Femoral artery and nerve should be in view to prevent accidental vascular or nerve injury.
Place a skin wheal at injection site.
Introduce the needle lateral to medial in-plane to the probe and advance the needle steeply into the trough, just lateral to the psoas tendon
After aspiration, inject anesthetic to visualize lifting of the psoas tendon off the bone and a plane of anesthetic just above the pelvic bone. If resistance is met at this step, try twisting your needle tip. If continued resistance is met, withdraw needle slightly
Place a skin wheal at injection site.
References
- Hematoma (fracture) block is safe and effective way to provide analgesia to a patient with a fracture.
- Very few contraindications exist for this block (overlying infection, medication allergy).
- Hematoma blocks can be utilized in any patient with a fracture requiring anesthesia or analgesia (ie before reduction), so long as local anesthetic can be safely infiltrated into the area. It is commonly utilized for forearm (Colle’s) fractures.
- When injecting local anesthetic for a fracture, ultrasound can help localize the fracture line and the block is most successful with the fracture line, rather than the hematoma, is targeted.