Erector Spinae Nerve Block
Welcome to the Erector Spinae Nerve Block regional anesthesia page. Here we will cover indications, contraindications, materials and steps for you to master this procedure. Let’s begin with the overview below.
Overview
The erector spinae is actually a group of muscles involved in maintaining an upright posture and rotating the back. The muscle group is composed of the iliocostalis, longissimus, and spinalis muscles.[1] These muscles run from the spinous process of the vertebrae out laterally to the transverse process and have connections on the ipsilateral ribs as well. The block is a fascia block, with deposition ideally under the fascia of the erector spinae muscle. This block is used for a variety of painful conditions of the torso.[2] While its exact mechanism is not clearly understood, it is thought to likely work by interfascial spread of local anesthetic toward the posterior rami of spinal nerves. In Emergency Medicine, it is commonly used for post-traumatic pain or to facilitate procedures such as chest tube placement.
Indications
Anesthesia of the anterior, lateral, and posterior regions of the chest and abdomen. As a relatively new block technique (first described in 2016), the indications for this procedure are less robustly delineated than other regional anesthesia techniques. That said, it has been used for a variety of painful conditions or procedures of the torso including rib fractures, percutaneous nephrolithotomies, even thoracotomies.[3] For Emergency Department patients, the block is often considered for rib fractures and pigtail / chest tube placement.
Contraindications
True contraindications to this block include:
- Infection (cellulitis) at the site of injection
- Allergy to local anesthetic being used
- Patient refusal
Some relative contraindications to consider are:
- Anticoagulation use or bleeding disorder should be noted and weighed in a risk/benefit manner. Not typically cited as a true contraindication
Anatomy
Depending on where along the thorax the regional anesthesia will be done, overlying muscles will vary. The erector spinae muscle is found directly superficial to the transverse process.
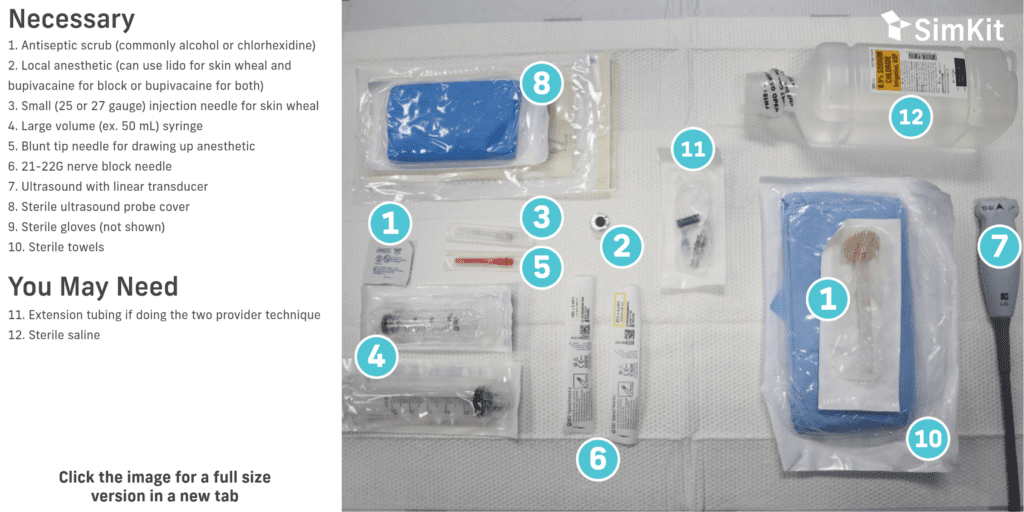
Materials

Technique
Blocks should be performed with aseptic technique using a skin antiseptic, sterile field, and sterile equipment (i.e. ultrasound) if possible. Allow appropriate dry time for your antiseptic. Block needles should be aspirated prior to every injection to avoid intravascular administration, and injection should be immediately stopped if the patient suddenly complains of pain or high pressure.
Procedure with step-by-step process
- Have the patient in a sitting position. The patient can rest the contralateral side against the stretcher brought into a 90 degree head up position.
- Clean the area with antiseptic solution and drape the area with sterile towels.
- Place the linear (or curvilinear) probe along the midline back oriented in the cephalad-caudad plane.
- Identify the spinous process and slide the probe toward the desired side of anesthesia until the transverse process is identified. Pan back and forth in this region to identify the overlying musculature and the erector spinae muscle.
- Place a skin wheal at injection site.
- Introduce the needle in-plane to the probe and advance the needle to puncture through the erector spinae muscle over the transverse process.
- After negative aspiration, inject anesthetic to perform hydrodissection and visualize deposition of anesthetic under the fascia of the erector spinae muscle.
- Continue to inject remaining anesthetic (20-40mL total) and confirm by visualizing expanding anechoic fluid.

Two Provider Technique
- Connect the extension tubing to the nerve block needle and to the syringe with local anesthetic.
- Prime the extension tubing with anesthetic to remove air.
- Perform Steps 1-5, as above.
- Perform the remaining steps with the first provider positioning the ultrasound probe and nerve block needle, and the second provider aspirating and injecting the anesthetic.
Summary & Bullet Points
References
[1] Erector Spinae Plane Nerve Block. NYSORA, Inc. Retrieved April 20, 2023, from https://www.nysora.com/erector-spinae-plane-block/
[2] Jain K, Jaiswal V, Puri A. Erector spinae plane block: Relatively new block on horizon with a wide spectrum of application – A case series. Indian J Anaesth. 2018 Oct;62(10):809-813. doi: 10.4103/ija.IJA_263_18. PMID: 30443066; PMCID: PMC6190410.
[3] Krishnan S, Cascella M. Erector Spinae Plane Block. [Updated 2023 Jan 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545305/
Erector Spinae Nerve Block
Overview
Indications
True contraindications to this block include:
- Infection (cellulitis) at the site of injection
- Allergy to local anesthetic being used
- Patient refusal
Some relative contraindications to consider are:
- Anticoagulation use or bleeding disorder should be noted and weighed in a risk/benefit manner. Not typically cited as a true contraindication
Anatomy
Materials
Technique
Procedure
Have the patient in a sitting position. The patient can rest the contralateral side against the stretcher brought into a 90 degree head up position.
Clean the area with antiseptic solution and drape the area with sterile towels.
Place the linear (or curvilinear) probe along the midline back oriented in the cephalad-caudad plane.
Identify the spinous process and slide the probe toward the desired side of anesthesia until the transverse process is identified. Pan back and forth in this region to identify the overlying musculature and the erector spinae muscle.
Place a skin wheal at injection site.
Introduce the needle in-plane to the probe and advance the needle to puncture through the erector spinae muscle over the transverse process.
After negative aspiration, inject anesthetic to perform hydrodissection and visualize deposition of anesthetic under the fascia of the erector spinae muscle.
Continue to inject remaining anesthetic (20-40mL total) and confirm by visualizing expanding anechoic fluid.
Two Provider Technique
- Connect the extension tubing to the nerve block needle and to the syringe with local anesthetic.
- Prime the extension tubing with anesthetic to remove air.
- Perform Steps 1-5, as above.
- Perform the remaining steps with the first provider positioning the ultrasound probe and nerve block needle, and the second provider aspirating and injecting the anesthetic.
Summary & Bullet Points
- Erector Spinae nerve block is a safe and effective way to provide analgesia for the torso
- Very little contraindications (overlying infection, medication allergy) exist for this procedure
- Erector Spinae blocks can reduce pain from trauma (rib fractures) or procedures (chest tube placement)
References
[1] Erector Spinae Plane Nerve Block. NYSORA, Inc. Retrieved April 20, 2023, from https://www.nysora.com/erector-spinae-plane-block/
[2] Jain K, Jaiswal V, Puri A. Erector spinae plane block: Relatively new block on horizon with a wide spectrum of application – A case series. Indian J Anaesth. 2018 Oct;62(10):809-813. doi: 10.4103/ija.IJA_263_18. PMID: 30443066; PMCID: PMC6190410.
[3] Krishnan S, Cascella M. Erector Spinae Plane Block. [Updated 2023 Jan 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545305/