Central Line Procedure
Welcome to the Central Line procedure page. Here we will cover indications, contraindications, materials and steps for you to master this procedure. Let’s begin below with the procedure video.
Procedure Video
A. Indications
The most common indication for central access is the use of strong vasoactive agents (vasopressors), but many other indications exist including: use of concentrated medications or hyperalimentation, emergent (crash) access need, unstable/inconsistent peripheral access in the critically ill or other patients requiring serial blood draws, or central venous pressure [CVP] monitoring (falling out of favor).[1]
B. Contraindications
Management by less invasive means is a contraindication to central access. Most patients can be managed with peripheral IV [PIV]. It is also worth noting that peripheral pressors through a trusted line have been demonstrated to be safe.[2][3] Crash central access must also be weighed against intraosseous access on a patient to patient (patient characteristics) and provider to provider (comfort and skill set) level. Overlying infectious processes (cellulitis) or suspected vasculitis are also contraindications.
Other relative contraindications include: suspected proximal vascular injury, profound coagulopathy, distorted local anatomy, uncooperative patient, and patient’s whose goals of care are inconsistent with invasive procedures.
C. Materials
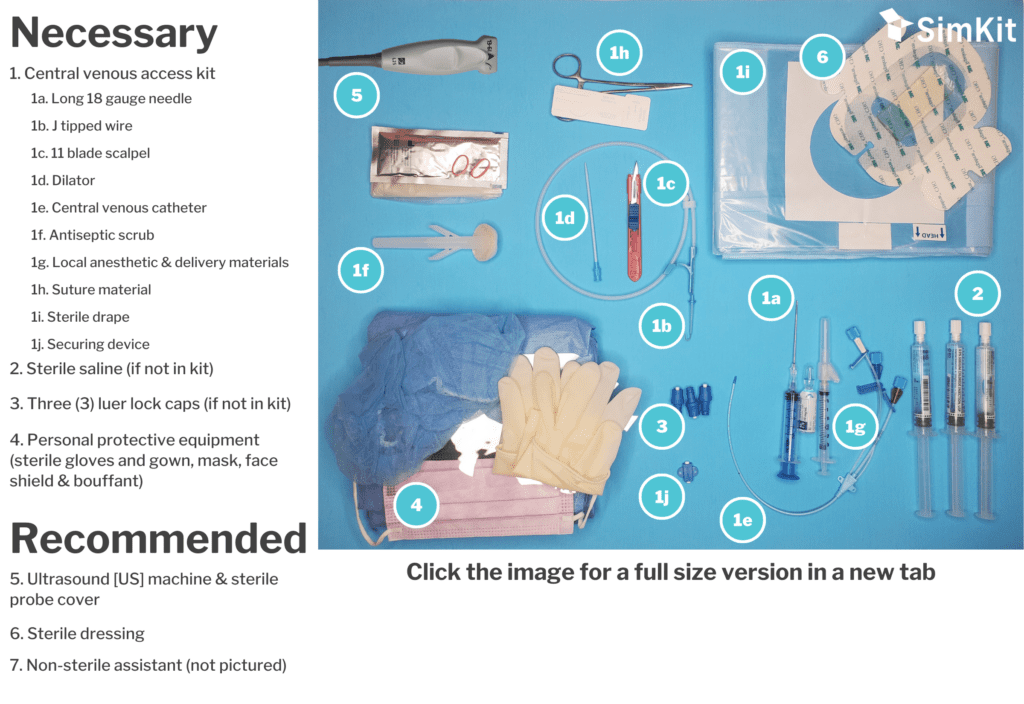
D. Steps
Step 1 | Determine the Ideal Site
For most indications, the preferred site is the one where the provider feels most comfortable and confident. That said, data suggest the subclavian site to be the preferred location to decrease thrombotic and infectious risk.[4] When done properly (and ideally under US guidance), this approach has comparable mechanical complication rates.[5][6][7] The right internal jugular (IJ) vein is another popular option. If US is going to be used for guidance, a non-sterile assessment of that site and visualization of landmarks can be helpful.
Note: Appropriate site is again going to depend on practitioner comfort, patient anatomy, as well as other factor such as anticoagulant use where a compressible site (right IJ) is preferred. The femoral vein is a secondary option when necessary, but carries a higher infection rate.
Step 2 | Position the Patient
Clear skin of leads, jewelry, or other equipment that may interfere with good sterile technique. Move IV poles/lines/vents/etc. from your work area. For IJ placement, the patient should be in trendelenburg. Be sure to ask a technician or nurse to be available to help redirect or gently restrain the patient if needed during the procedure. Orient your ultrasound machine so that it is in your direct line of sight.
Step 3 | Prepare Area, go Sterile
Step 4 | Prepare Equipment
Have a non-sterile assistant dump three luer lock caps and empty 30 mL of sterile saline into the central line tray if not pre-equipped. Flush each port of the catheter with sterile saline. Apply luer locks to side ports if using a triple lumen catheter, leaving the central port uncapped as this is where the guidewire will exit. Prepare equipment in the intended order of use, putting equipment within direct view of the operator, ideally so that they can be accessed without eyes being taken off the patient or procedure, in a space unaffected by patient movement (i.e. Mayo stand). Equipment to have prepared and ready: cannulating syringe, guidewire, scalpel, dilator, and catheter. If not done so already the, sterile probe cover can be applied to the US probe. If the patient is awake or aware of painful stimuli, anesthetize the area. Doing this under direct US guidance as a “dry run” of the procedure can be helpful.
Note: Avoid instilling any air with anesthetic as this can distort the US view.
Note: For subclavian access, anesthetizing the clavicle periosteum can be beneficial.
Step 5 | Cannulate and Insert Guidewire
If using US (recommended), guide your cannulating syringe into vessel. If the operator is comfortable, the longitudinal orientation of the US probe is preferred as the syringe can be visualized through the entire trajectory. This helps avoid passing beyond the target and into surrounding structures. When the needle tip is within the target vessel, drop the US probe and stabilize the needle with the non-dominant hand. Remove the syringe and grasp the guidewire, ideally without taking your eyes off the procedural field. Guide the guidewire into the needle and into the lumen of the vessel. It should glide without resistance when passing through the lumen of the vessel. If resistance is felt, gentle repositioning by rotating the needle and/or wire is warranted. If this does not alleviate the resistance, re-attaching the syringe to be sure blood can be aspirated and checking needle tip position with the ultrasound may be helpful. Avoid excessive force as this can kink the guidewire. When the wire advances freely into the needle and vessel, the needle can be guided off the far end of the wire. Use US to confirm the wire is indeed within the vessel.
Note: If the guidewire is not advancing, the whole apparatus (wire and needle) must be removed to avoid shearing off the wire.
Note: If the guidewire tickles the ventricle, you may see premature ventricular contractions (PVCs). If you see multiple PVCs, withdraw your guidewire 3-5 cm before proceeding.
Step 6 | Dilate
While avoiding taking your eyes off the field, grab your scalpel and make a skin nick. Orient the sharp side of your blade AWAY from the wire to avoid nicking the wire itself. In addition, be very careful to ensure the nick is contiguous with the wire entry site, avoiding any skin bridge. Then grasp your dilator and thread it over your wire. When at the skin, grab at the proximal end of the dilator and gently “rack” the wire, moving it back and forth 2-3 mm while advancing the dilator in a twisting fashion. Take care to hold the wire in position to avoid allowing the dilator to carry it further into the vessel lumen.
Note: this step is prone to kinking of the wire, which should be avoided. If significant resistance is felt with dilation, withdraw the dilator partially, rack the guidewire to confirm free movement, and re-advance the dilator in a twisting fashion.
Step 7 | Advance the Catheter
When dilation is complete, remove the dilator while holding firm to your wire and grasp your catheter. It is good practice to hold pressure with gauze at the insertion site to limit blood loss and hematoma formation while you retrieve and advance your catheter. Advance your catheter over the wire while slowly withdrawing the wire from the insertion site and feeding it into the catheter. Once the wire is thread through the entire catheter and can be grasped through the middle port, you can advance the catheter over the remaining wire. Take care to hold the wire tightly during this step to avoid the wire being carried into the vessel with the catheter. As with the dilator, advance the central line over the wire in a twisting fashion. It should advance smoothly, without resistance.
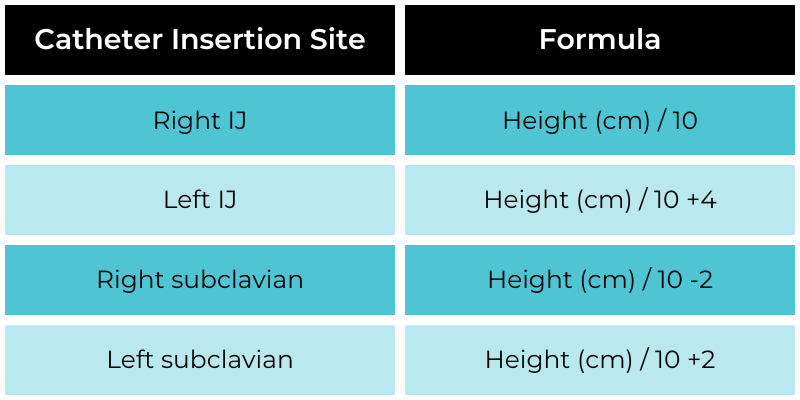
Note: Depending on the catheter length and desired tip location in the patient, the catheter may not need to be advanced fully. The following formulas can assist in guiding insertion depth. Chest X-ray (see table below) is used to confirm catheter tip location and adjustments can be made based on this imaging.
Step 8 | Confirm Blood Return
Fully remove the guidewire from the middle port of the catheter and apply the luer lock cap to the middle port. Using a saline filled syringe, aspirate the air from this port and confirm that blood can be withdrawn. Flush the port with saline and clamp closed. Aspirate any remaining air on the other two ports, also confirming that blood can be aspirated from each, flush and lock them as well. Again confirm placement in the intended vessel with your US. Use the included catheter anchoring devices to stabilize the line (classically white and blue) which can be clamped onto the catheter and sutured to the skin.
Step 9 | Clean-up and Confirm your Work
Remember the ICU only sees your end product. Clean the site of blood and apply a sterile dressing. Clean all sharps and other procedural materials and confirm line placement when appropriate (chest X-ray for IJ and subclavian lines) both to confirm placement and evaluate for pneumothorax.
References
[1] Hebert R, Bose S, Mace S. (2017). “Central venous catheterization and central venous pressure monitoring” in Roberts J. Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care. Elsevier.
[2] Pancaro C, Shah N, Pasma W, Saager L, Cassidy R, van Klei W, Kooij F, Vittali D, Hollmann MW, Kheterpal S, Lirk P. Risk of Major Complications After Perioperative Norepinephrine Infusion Through Peripheral Intravenous Lines in a Multicenter Study. Anesth Analg. 2019 Sep 27.
[3] Tian D, Smyth C, Keijzers G, Macdonald SP, Peake S, Udy A, Delaney A. Safety of peripheral administration of vasopressor medications: A systematic review. Emerg Med Australas. 2020 Apr;32(2):220-227.
[4] Parienti JJ, Mongardon N, Mégarbane B, Mira JP, Kalfon P, Gros A, Marqué S, Thuong M, Pottier V, Ramakers M, Savary B, Seguin A, Valette X, Terzi N, Sauneuf B, Cattoir V, Mermel LA, du Cheyron D; 3SITES Study Group. Intravascular Complications of Central Venous Catheterization by Insertion Site. N Engl J Med. 2015 Sep 24;373(13):1220-9.
[5] Palepu GB, Deven J, Subrahmanyam M, Mohan S. Impact of ultrasonography on central venous catheter insertion in intensive care. Indian J Radiol Imaging. 2009 Jul-Sep;19(3):191-8.
[6] Fragou M1, Gravvanis A, Dimitriou V, Papalois A, Kouraklis G, Karabinis A, Saranteas T, Poularas J, Papanikolaou J, Davlouros P, Labropoulos N, Karakitsos D. Real-time ultrasound-guided subclavian vein cannulation versus the landmark method in critical care patients: a prospective randomized study. Crit Care Med. 2011 Jul;39(7):1607-12.
[7] Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF. Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization. Cochrane Database Syst Rev. 2015 Jan 9;1:CD011447.
Central Line Procedure
Welcome to the Central Line procedure page. Here we will cover indications, contraindications, materials and steps for you to master this procedure. Let’s begin below with the procedure video.
Procedure Video
Indications
The most common indication for central access is the use of strong vasoactive agents (vasopressors), but many other indications exist including: use of concentrated medications or hyperalimentation, emergent (crash) access need, unstable/inconsistent peripheral access in the critically ill or other patients requiring serial blood draws, or central venous pressure [CVP] monitoring (falling out of favor).[1]
B. Contraindications
Management by less invasive means is a contraindication to central access. Most patients can be managed with peripheral IV [PIV]. It is also worth noting that peripheral pressors through a trusted line have been demonstrated to be safe.[2][3] Crash central access must also be weighed against intraosseous access on a patient to patient (patient characteristics) and provider to provider (comfort and skill set) level. Overlying infectious processes (cellulitis) or suspected vasculitis are also contraindications.
Other relative contraindications include: suspected proximal vascular injury, profound coagulopathy, distorted local anatomy, uncooperative patient, and patient’s whose goals of care are inconsistent with invasive procedures.
C. Materials
References
[1] Hebert R, Bose S, Mace S. (2017). “Central venous catheterization and central venous pressure monitoring” in Roberts J. Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care. Elsevier.
[2] Pancaro C, Shah N, Pasma W, Saager L, Cassidy R, van Klei W, Kooij F, Vittali D, Hollmann MW, Kheterpal S, Lirk P. Risk of Major Complications After Perioperative Norepinephrine Infusion Through Peripheral Intravenous Lines in a Multicenter Study. Anesth Analg. 2019 Sep 27.
[3] Tian D, Smyth C, Keijzers G, Macdonald SP, Peake S, Udy A, Delaney A. Safety of peripheral administration of vasopressor medications: A systematic review. Emerg Med Australas. 2020 Apr;32(2):220-227.
[4] Parienti JJ, Mongardon N, Mégarbane B, Mira JP, Kalfon P, Gros A, Marqué S, Thuong M, Pottier V, Ramakers M, Savary B, Seguin A, Valette X, Terzi N, Sauneuf B, Cattoir V, Mermel LA, du Cheyron D; 3SITES Study Group. Intravascular Complications of Central Venous Catheterization by Insertion Site. N Engl J Med. 2015 Sep 24;373(13):1220-9.
[5] Palepu GB, Deven J, Subrahmanyam M, Mohan S. Impact of ultrasonography on central venous catheter insertion in intensive care. Indian J Radiol Imaging. 2009 Jul-Sep;19(3):191-8.
[6] Fragou M1, Gravvanis A, Dimitriou V, Papalois A, Kouraklis G, Karabinis A, Saranteas T, Poularas J, Papanikolaou J, Davlouros P, Labropoulos N, Karakitsos D. Real-time ultrasound-guided subclavian vein cannulation versus the landmark method in critical care patients: a prospective randomized study. Crit Care Med. 2011 Jul;39(7):1607-12.
[7] Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF. Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization. Cochrane Database Syst Rev. 2015 Jan 9;1:CD011447.