Which central line is best? I would argue we all have our “go to” line, which across the country is likely the ultrasound (US) guided internal jugular or IJ. Well, considering common circumstances encountered by Emergency Medicine (EM) clinicians, what does the literature say is likely the best line??
To answer this question let’s dive into the literature… I think you’ll be surprised by what we find.
Society Recommendations
Between the IJ, subclavian, and femoral line, when everything else is equal, which is recommended by professional organizations?
The Center for Disease Control and Prevention (CDC) makes the following recommendation:
“Use a subclavian site, rather than a jugular or a femoral site, in adult patients to minimize infection risk for non-tunneled CVC placement. [Category IB]“
Where does this recommendation come from? They base it on three studies: [Merrer 2001, Goetz 1998, Robinson 1995].
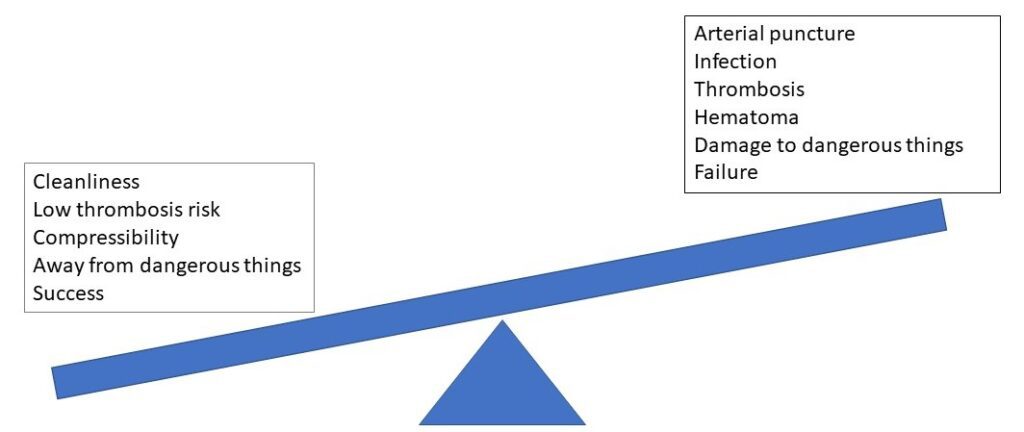
This analysis brings up a more global point that for each line and site we need to weigh the risks and benefits. These potential risks and benefits are shown in the figure below:
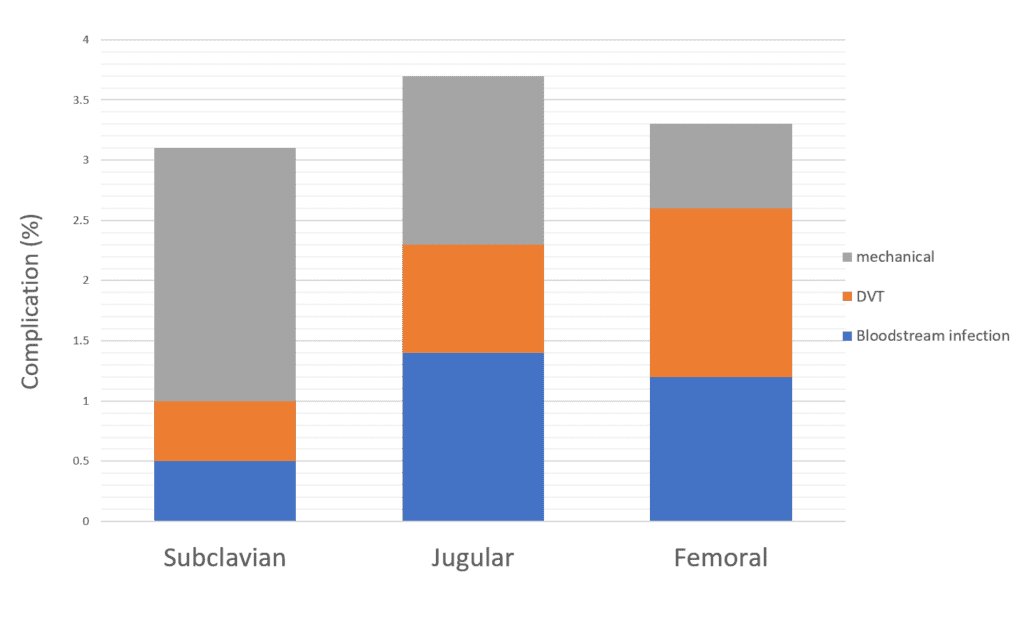
Aside from the CDC recommendation, what other data do we have to guide our decisions on what site is best? The most valuable data on the topic comes from the 3 SITES Study by Parienti in the New England Journal of Medicine (2015). They compared the IJ to subclavian to femoral in a 1:1:1 randomization fashion. When looking at complications, they found the following:
The subclavian line had the lowest overall complication rate at just above 3%. As you can see, the majority of these were mechanical.
Enter Ultrasound Guidance
What if we could decrease the mechanical complication rate with a skillset we already have? What if the graph looked more like this?
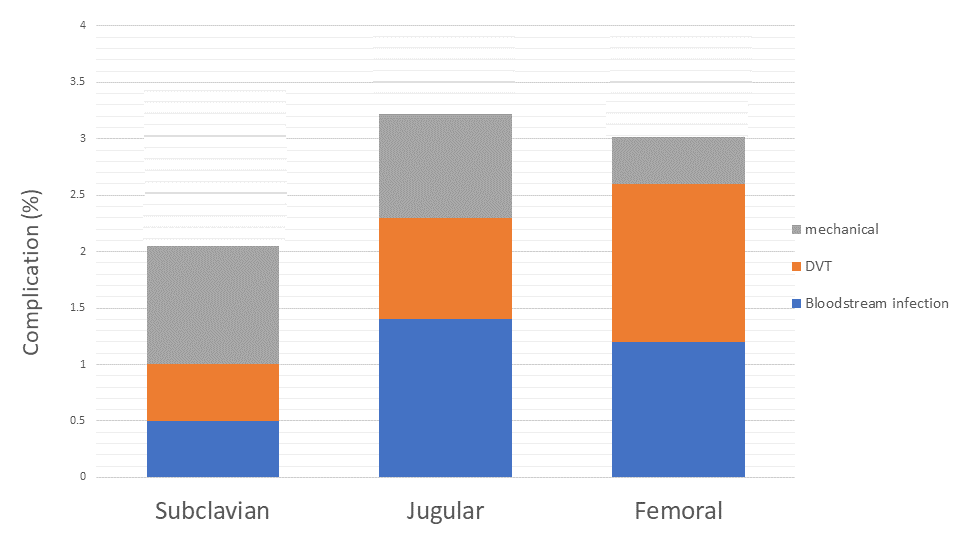
Notice how all three have a decrease in mechanical complication rate, but it is the subclavian’s much lower thrombotic and blood stream infection rates that really lead to the difference. The use of ultrasound can achieve this in the right setting and with the correct skill set. This is supported by the literature.
A Cochrane Review in 2015 reviewed 9 articles on the use of US for subclavian lines, 5 of which involved 2 dimensional US (4 using doppler only). In their review they concluded:
“US offers small gains in safety and quality when compared to landmark technique.”
While this is not a glowing review, I think it likely under estimates the true benefit in modern practice, we we are getting way more comfortable with US and much less facile with landmark or anatomy-based procedures.
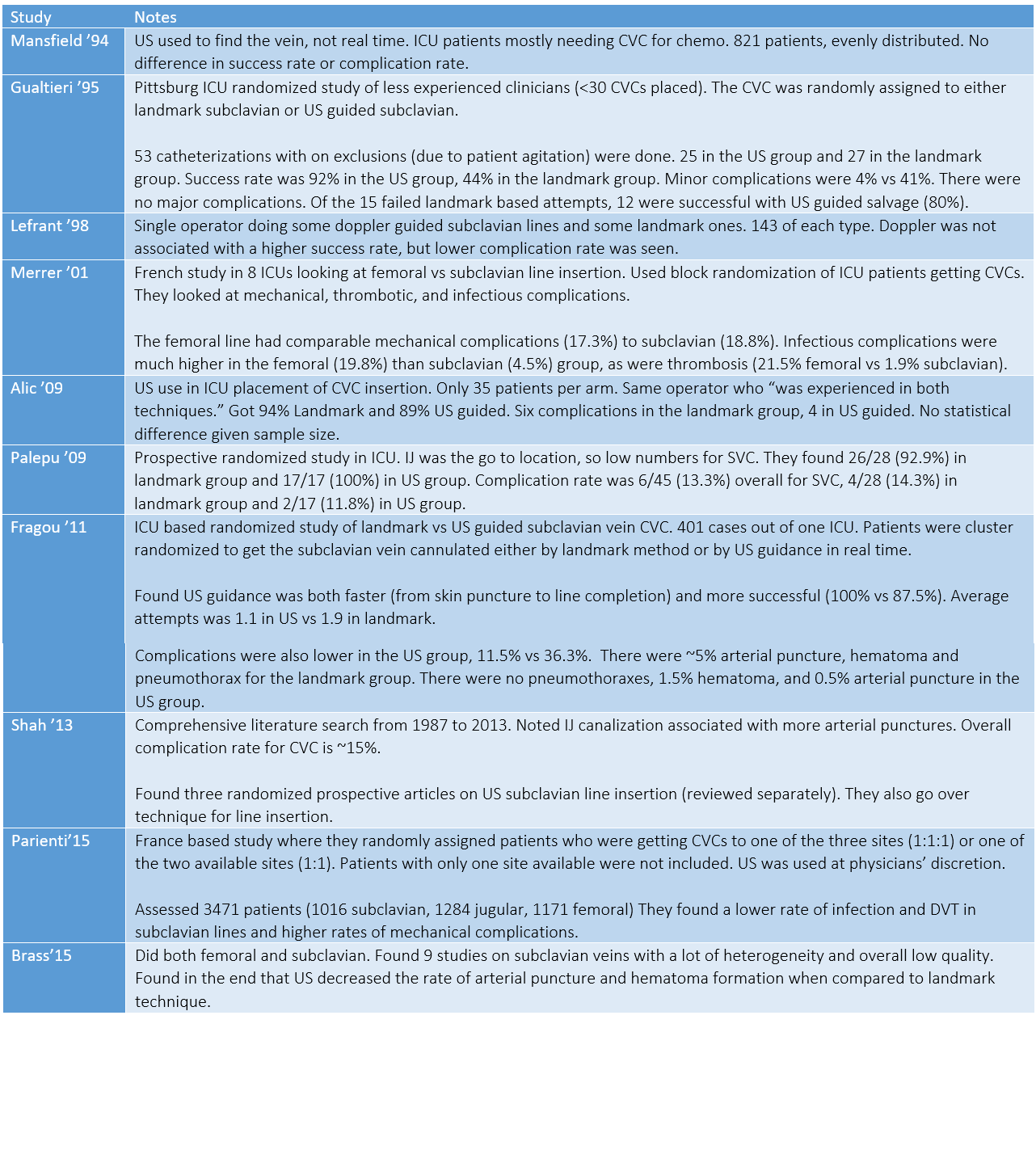
Some of the relevant supporting literature for US guided subclavian line is summarized in the table below. See reference list below for all studies.
How to Perform an US Guided Subclavian Central Line
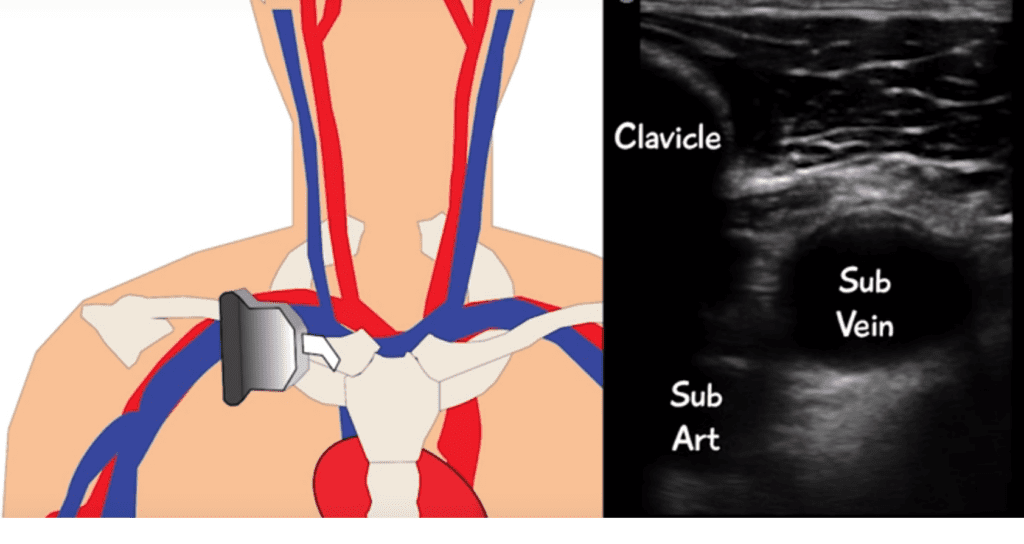
The secret to the US-guided subclavian CVC is to look much more laterally than the landmark technique. In the landmark approach, we are finding the junction of the middle and medial thirds of the clavicle, then sneak our needle in under the bone to hit the subclavian vein.
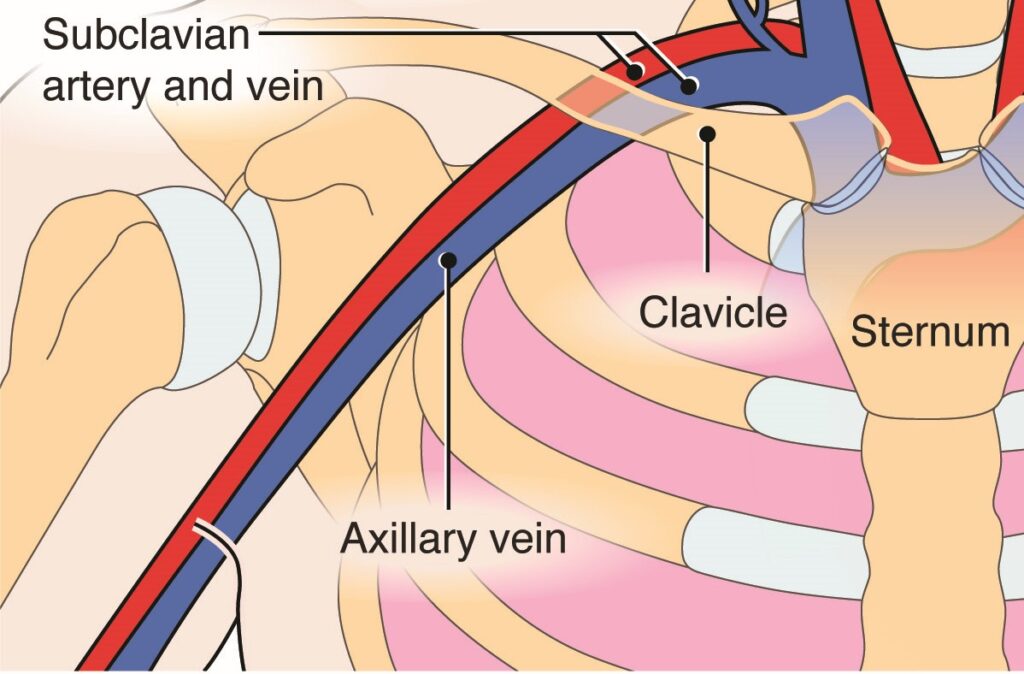
In our US-guided approach, we start laterally to identify the axillary vein and find our ideal venipuncture site from there, sometimes even cannulating the axillary vein itself (remember the vessel changes names as it crosses over the 1st rib).
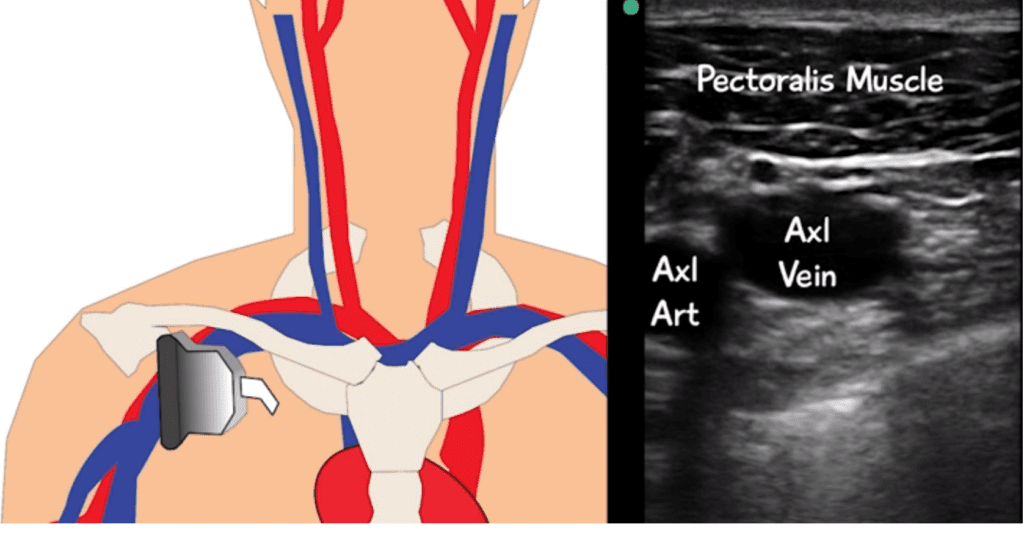
The axillary cannulation has the advantage of often being separated from the pleura more than the subclavian. It also has not yet begun to dive under the clavicle. If you are capable, a longitudinal approach is often recommended as an additional safeguard against pleura injury.
Here is a video of a subclavian CVC placed under US guidance in the longitudinal plane.
And to show you this is not just a handful of people who have this anatomy, here is my own axillary vein becoming the subclavian. It is pretty easy to spot where to cannulate the vein just before the clavicle comes into view.
Additional Moves
PART
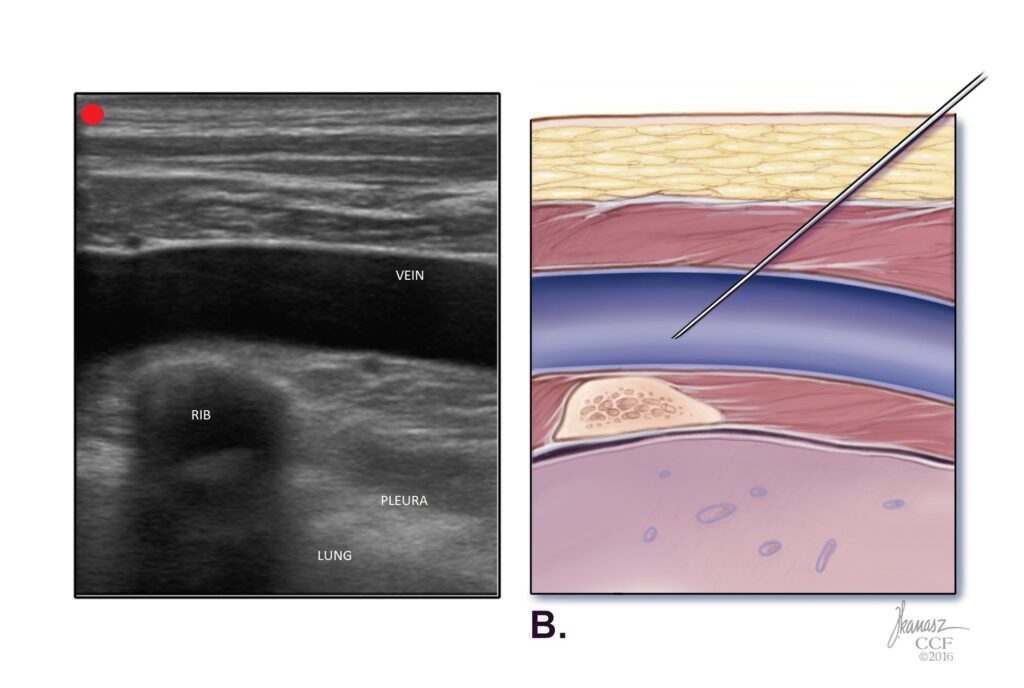
For additional safety, Dr. Senussi et al recommend the Pleural Avoidance with Rib Trajectory (PART) technique. In doing this, the operator attempts to cannulate the subclavian vein (really the axillary vein) in a region that has a rib as a backstop. In their paper they discuss the use of the second rib for this purpose. This is definitely a pro move that requires a far bit of knowledge of anatomy and skill in ultrasound.
SHRUG technique from PULMCrit
With the shrug technique, a conscious patient shrugs their shoulders upward, pulling it up and out of the way of venous cannulation. This positioning can be replicated in the less-than-cooperative or unconscious patient by bracing the patient’s elbow upward for shrug position.
A Final Thought on Landmark Technique Subclavian
While blind subclavian lines are far from ideal, in a truly emergent situation they can be life saving. It is worth noting that an alterative to the traditional infraclavicular approach exists in the supraclavicular approach, or “pocket shot.” In this approach you are feeling the lateral head of the sternocleomastoid (SCM) muscle and its connection to the clavicle. Right at that connection point there is a soft indent into the neck, termed “the pocket.” After finding the pocket, you insert your needle 1 cm lateral to the SCM muscle and 1 cm posterior to the clavicle, aiming for the contralateral nipple. A 2020 Meta-analysis of eight RCTs found this approach to be superior to the blind infraclavicular approach.
For more on this approach, check out this review article.
Conclusions
1. The subclavian vein has been shown with a reasonable degree of quality evidence to have the lowest risks of infection and thrombosis.
2. Mechanical complications plague the placement of a subclavian line, which can be overcome by ultrasound.
3. The US guided subclavian is made easier by:
- Looking out toward the axillary vein for actual canulation
- Using a rib to protect against puncturing the pleura
- Having the patient shrug
4. If doing a blind subclavian, the supraclavicular approach may be better… in the right hands.
Keeping your skills sharp is an uphill battle. Let SimKit do the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. We want you to be confident and competent clinicians, and we have the tools to help.
References & Additional Readings
Mansfield PF1, Hohn DC, Fornage BD, Gregurich MA, Ota DM. Complications and failures of subclavian-vein catheterization.N Engl J Med. 1994 Dec 29;331(26):1735-8. [pubmed]
Gualtieri E, Deppe SA, Sipperly ME, Thompson DR. Subclavian venous catheterization: greater success rate for less experienced operators using ultrasound guidance. Crit Care Med. 1995 Apr;23(4):692-7. [pubmed]
Lefrant JY, Cuvillon P, Bénézet JF, Dauzat M, Peray P, Saïssi G, de La Coussaye JE, Eledjam JJ. Pulsed Doppler ultrasonography guidance for catheterization of the subclavian vein: a randomized study. Anesthesiology. 1998 May;88(5):1195-201. [pubmed]
Palepu GB, Deven J, Subrahmanyam M, Mohan S. Impact of ultrasonography on central venous catheter insertion in intensive care. Indian J Radiol Imaging. 2009 Jul-Sep;19(3):191-8. [pubmed]
Fragou M1, Gravvanis A, Dimitriou V, Papalois A, Kouraklis G, Karabinis A, Saranteas T, Poularas J, Papanikolaou J, Davlouros P, Labropoulos N, Karakitsos D. Real-time ultrasound-guided subclavian vein cannulation versus the landmark method in critical care patients: a prospective randomized study. Crit Care Med. 2011 Jul;39(7):1607-12. [pubmed]
Merrer J1, De Jonghe B, Golliot F, Lefrant JY, Raffy B, Barre E, Rigaud JP, Casciani D, Misset B, Bosquet C, Outin H, Brun-Buisson C, Nitenberg G; French Catheter Study Group in Intensive Care. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001 Aug 8;286(6):700-7. [pubmed]
Shah A, Smith A, Panchatsharam S. Ultrasound-guided subclavian venous catheterisation – is this the way forward? A narrative review. Int J Clin Pract. 2013 Aug;67(8):726-32. [pubmed]
Parienti JJ, Mongardon N, Mégarbane B, Mira JP, Kalfon P, Gros A, Marqué S, Thuong M, Pottier V, Ramakers M, Savary B, Seguin A, Valette X, Terzi N, Sauneuf B, Cattoir V, Mermel LA, du Cheyron D; 3SITES Study Group. Intravascular Complications of Central Venous Catheterization by Insertion Site. N Engl J Med. 2015 Sep 24;373(13):1220-9. [pubmed]
Brass P, Hellmich M, Kolodziej L, Schick G, Smith AF. Ultrasound guidance versus anatomical landmarks for subclavian or femoral vein catheterization. Cochrane Database Syst Rev. 2015 Jan 9;1:CD011447. [pubmed]
Goetz AM1, Wagener MM, Miller JM, Muder RR. Risk of infection due to central venous catheters: effect of site of placement and catheter type. Infect Control Hosp Epidemiol. 1998 Nov;19(11):842-5. [pubmed]
Robinson JF, Robinson WA, Cohn A, Garg K, Armstrong JD, 2nd. Perforation of the great vessels during central venous line placement. Arch Intern Med 1995; 155:1225–8. [pubmed]
Senussi MH, Kantamneni PC, Omranian A, Latifi M, Hanane T, Mireles-Cabodevila E, Chaisson NF, Duggal A, Moghekar A. Revisiting Ultrasound-Guided Subclavian/Axillary Vein Cannulations: Importance of Pleural Avoidance With Rib Trajectory. J Intensive Care Med. 2017 Jul;32(6):396-399. [pubmed]
Chen Q, Long Q, Liang JQ, Tang TX, Yang B. Comparative evaluation of the clinical safety and efficiency of supraclavicular and infraclavicular approaches for subclavian venous catheterization in adults: A meta-analysis. The American Journal of Emergency Medicine 38.7 (2020): 1475-1480. [pubmed]
Subscribe to the Podcast on



Podcast subscription form
"*" indicates required fields