Hi, my name is Jason Hine. I’m an emergency medicine physician and the founder of SimKit. Today we’re going to be reviewing the Gastroesophageal Balloon Tamponade devices: the Linton, Minnesota and Blakemore tubes.
Now while these devices give many a well-meaning practitioner pause and palpitations. They really are relatively simple in their design, and most of that anxiety comes from our own lack of familiarity with them. We can overcome that by reviewing these devices now.
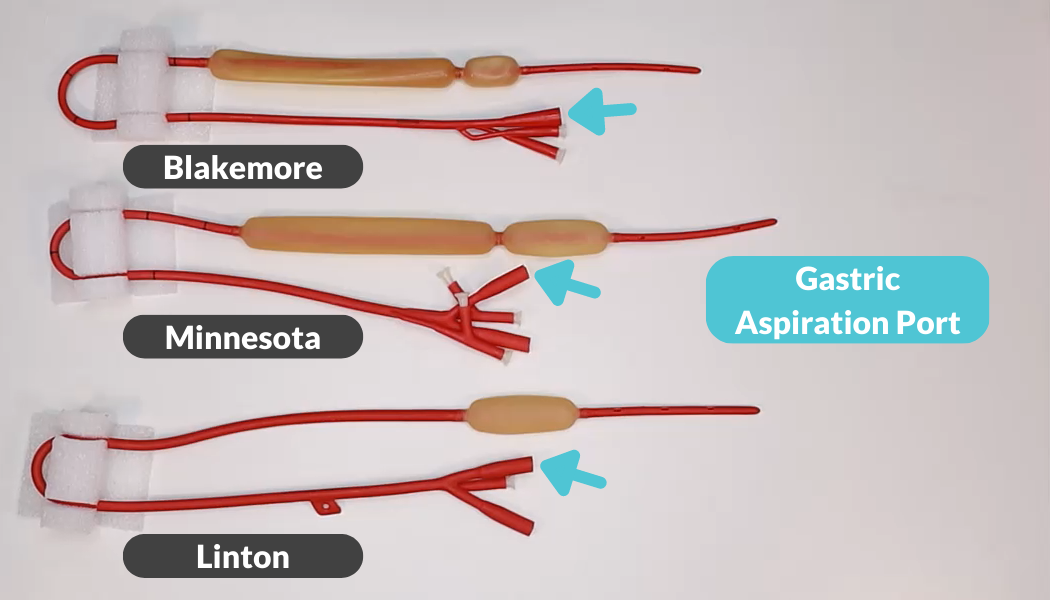
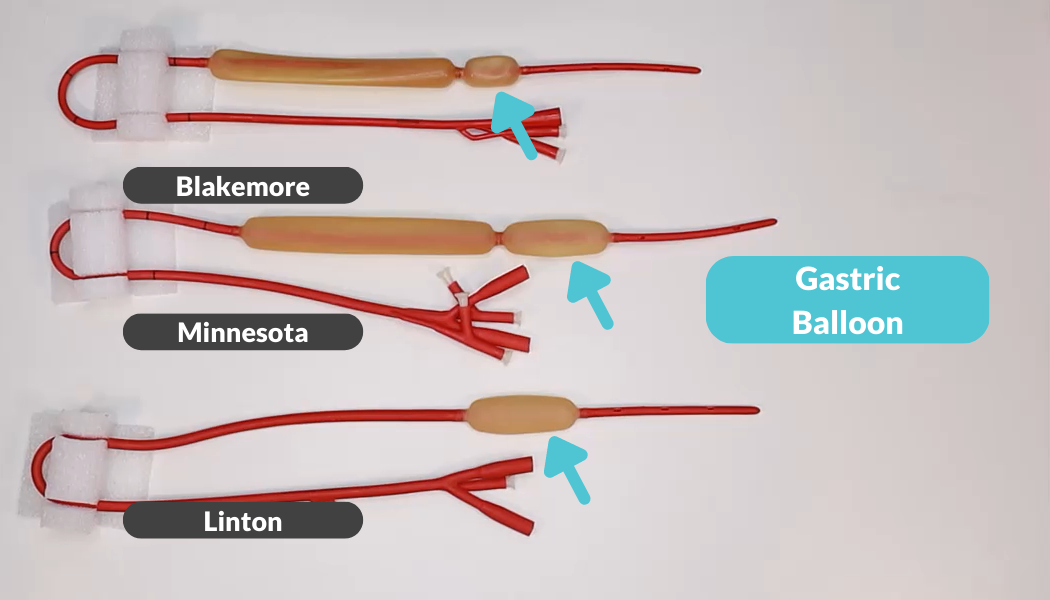
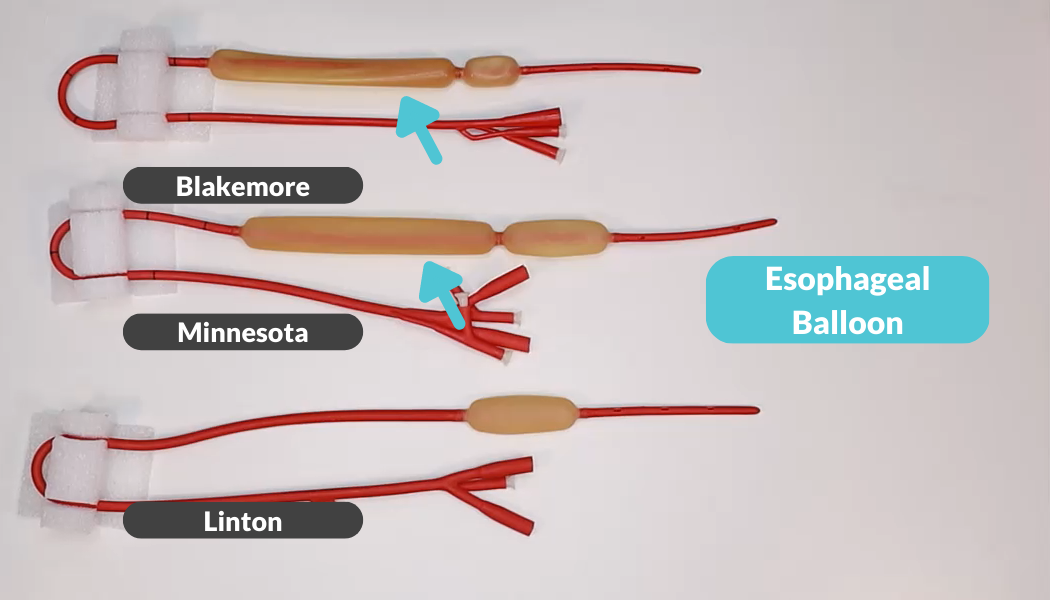
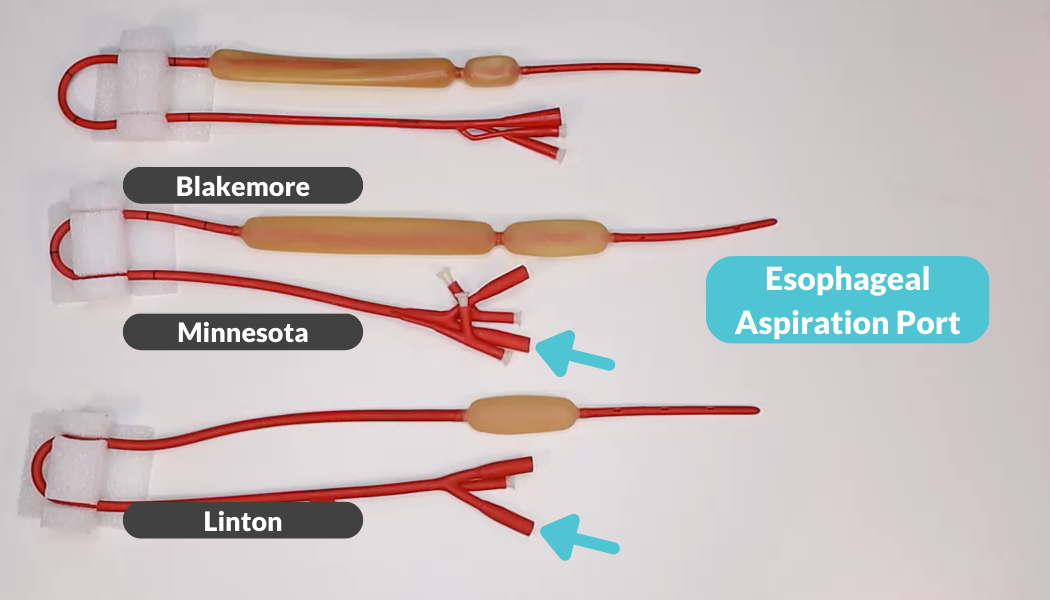
Here we have laid out our three different types of gastroesophageal balloon tamponade devices: the Linton, the Minnesota, and the Blakemore tube. These three tubes actually have many parts in common. They all have a gastric aspiration port, and a gastric balloon. The Linton and Minnesota tube have esophageal aspiration ports and the Minnesota and Blakemore tube have esophageal balloons. And that’s really it. That’s the anatomy of these tubes.
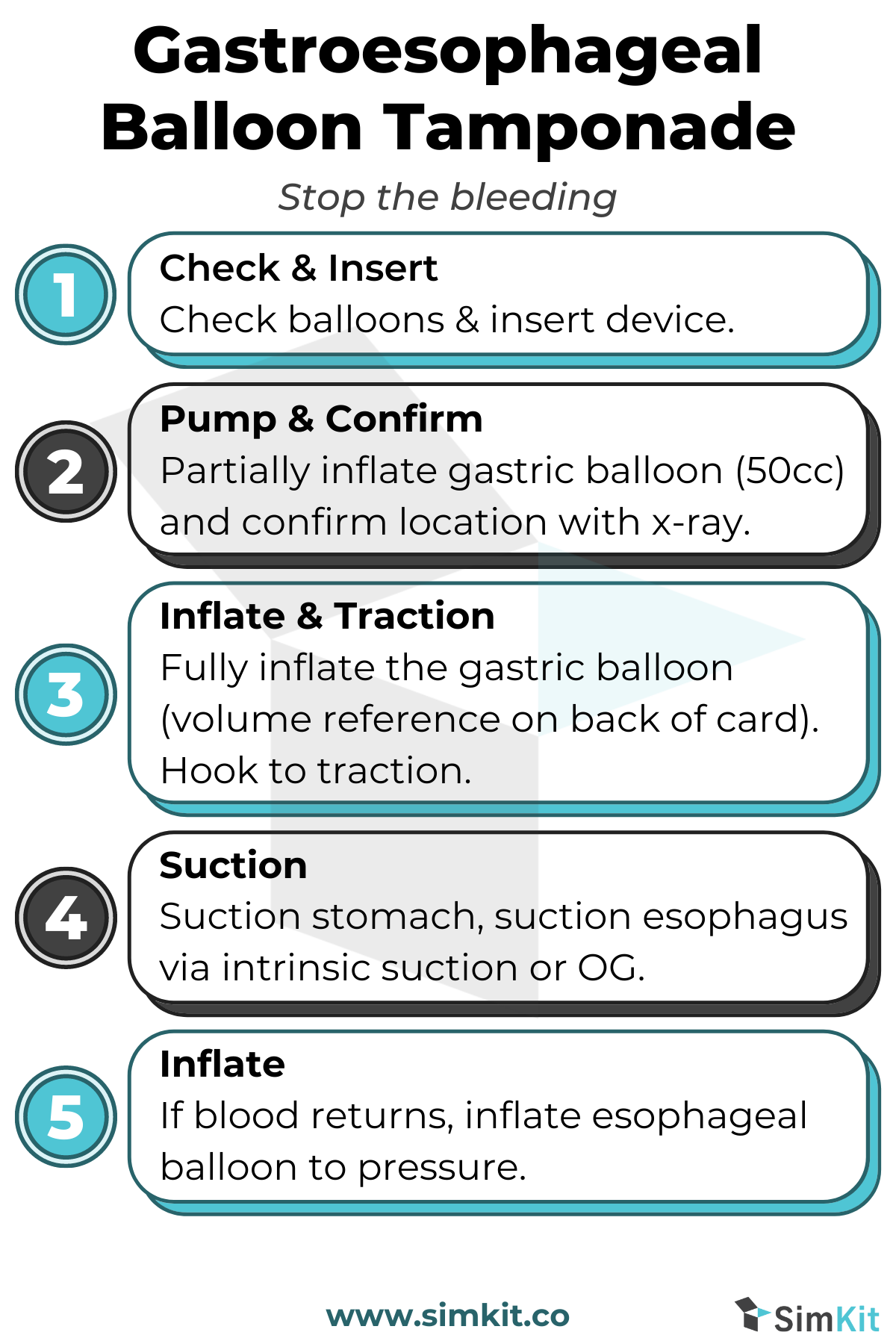
Now let’s go through the process of unpackaging and inserting a gastroesophageal balloon tamponade device. First thing we want to do is be familiar with the packaging. They all come in these boxes. Inside the box is a plastic bag and a Styrofoam holder. Once it’s taken out of the holder, that box can be discarded. The next thing we want to recognize are these little plastic plungers that are not hollow bore on the end of all the balloon ports. They are going to be removed and they’re kind of spot welded in place and a little difficult to take off. Now, taking a look at the Linton tube first, we see our gastric aspiration fenestrations there and our gastric balloon right here. Above the gastric balloon we see the fenestrations for esophageal aspiration. Here we can remove these spot-welded on plungers, which again are not hollow bore and do not allow any passage of air.
We have the Minnesota tube in all its glory. We have our gastric balloon here and the fenestrations for gastric aspiration below that. Looking higher up on the tube, we see our holes for esophageal aspiration above our esophageal balloon. Now, like the Linton tube it has two areas where we can aspirate, we have two ports for aspiration labeled for gastric and esophageal ASP. Here’s an area where the Minnesota tube is slightly different in that each port has two holes for insufflation of air. We are going to remove the stoppers from ONE of these each.
Now finally, we have the Blakemore tube. Like the others, it has a gastric balloon and gastric fenestrations for aspiration. All three share that in common. It, like the Minnesota tube, has an esophageal balloon. It does NOT have esophageal aspiration ports. As with the others, we can remove the plastic stoppers from the insufflation ports.
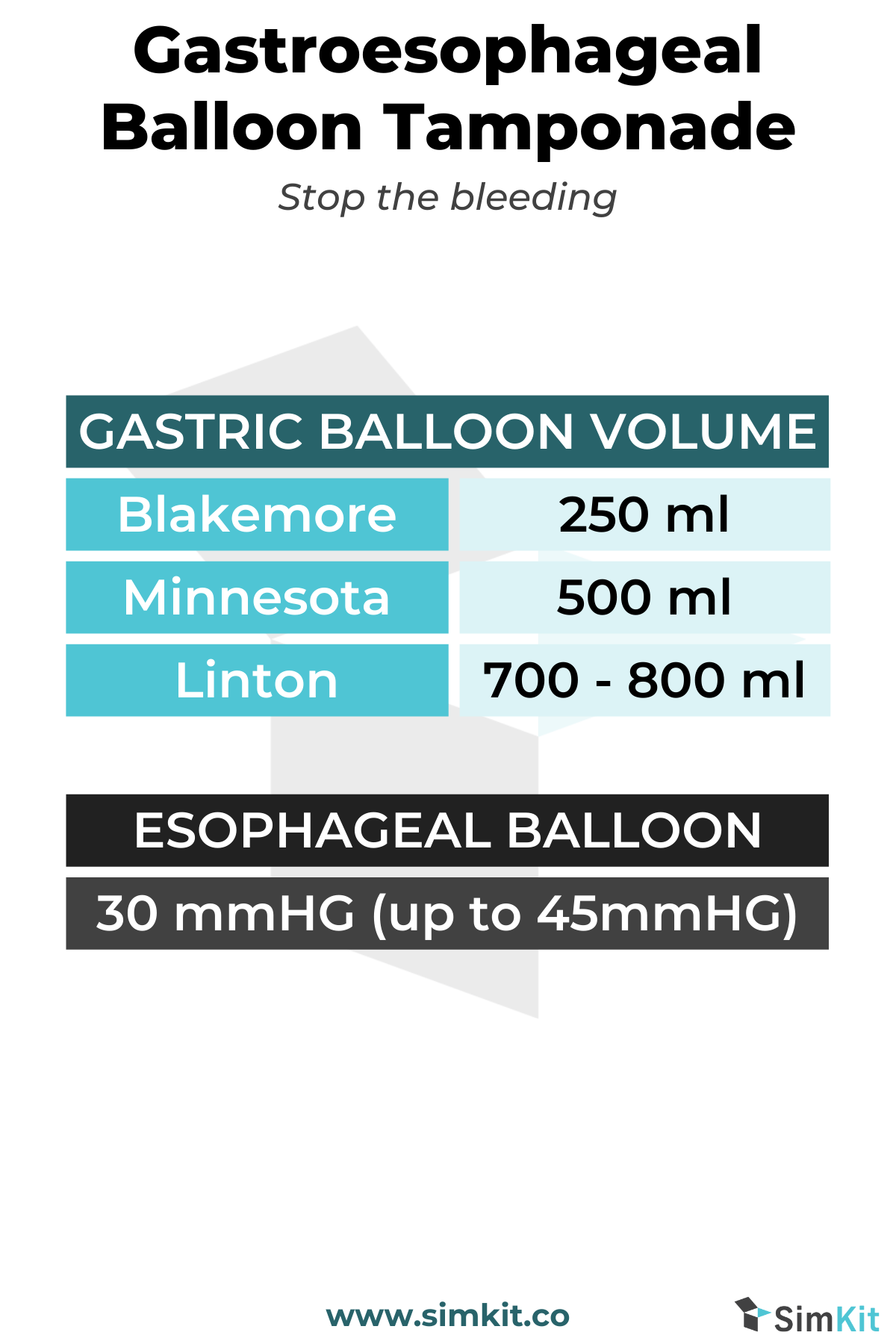
Now let’s talk about volume for our gastric balloons. The Linton tube takes 700 to 800 mL, the Minnesota 500 mL and the Blakemore 250 mL. For the esophageal balloons on the Minnesota and the Blakemore, they are not by volume but by pressure. They are going to take 30 mmHg pressure and can be inflated up to 45 if needed to stop bleeding. Our final point to remember is that the Blakemore tube does not have fenestrations for a soft you aspiration. The solution for this if you want to see if there’s bleeding in the esophagus is to place an NG or OG tube down into the esophageal area and aspirate for blood. If blood is seen, the esophageal balloon should be inflated.
And there you have it, these three tubes demystified. Be sure to check out the show notes for helpful tables and infographics.