Lateral Canthotomy 1
History
Orbital compartment syndrome (OCS) leading to blindness was first published on in Plastics and Reconstructive Surgery in 1950.[1] From here, lateral canthotomy was established as an operative procedure, with early accounts of drains being placed to help aid in decompression. For many subsequent years, the procedure was reserved for the operative suite and not considered within the Emergency Medicine provider’s scope of practice.[2] Through advancing medical technologies and concurrent modification and simplification of the procedure, lateral canthotomy has come into the Emergency Medicine physician’s scope of practice. In 1981, the first ED-based lateral canthotomy was documented.[3]
Anatomy
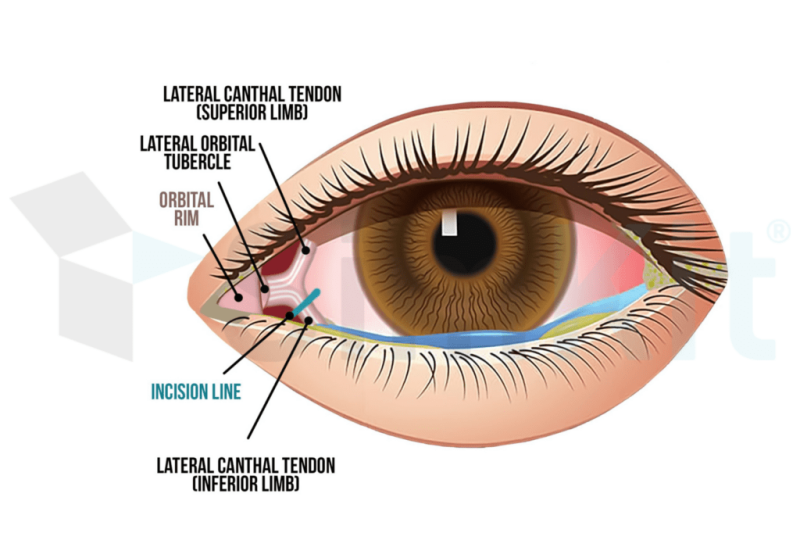
The orbital compartment is a complex and compact area of anatomy, containing many nerves (most notably the optic nerve), muscle bellies and their associated tendons, and blood vessels. The eye is held in the socket in part by the inferior and superior orbital septa and their associated attachment points including the medial and lateral canthi. When blood accumulates in the orbital compartment (i.e. from a retrobulbar hematoma), it rapidly increases the pressure on structures contained within. Other causes of OCS include intraocular hematoma, sub-periosteal hematoma, and sinus fractures with orbital emphysema. Outside of trauma, the most common causes of OCS are facial surgery and orbital cellulitis.[5][6] When the optic nerve is compressed, injury can occur quickly, and current literature notes improved visual outcomes when intervention is completed within two hours.[7]
To release the pressure, the lateral canthus with its component inferior and superior crus are cut, allowing for anterior protrusion of the eye and other orbital compartment content.
Indications
Lateral canthotomy is reserved for acute OCS. Causes of acute OCS are discussed above in the Anatomy section. With acute OCS, patients will note pain, limited eye movement, and visual impairment varying from decreased or blurry vision to full vision loss. In the setting of pathologic anatomical changes causing a potential for acute OCS (ex: retrobulbar hematoma), orbital compartment syndrome is diagnosed clinically. Signs of acute OCS include proptosis, decreased visual acuity in the affected eye, limited extraocular movement, afferent pupillary defect, and increased intraocular pressure.[8]
If there is diagnostic uncertainty or additional data points are desired, intraocular pressure measurement with a soft cut point of 40 mmHg is often used to further support the need for lateral canthotomy in addition to clinical features.
Contraindications
The only absolute contraindication to lateral canthotomy is globe rupture. This can be diagnosed clinically or by imaging (CT).
Equipment
Betadine or other antiseptic, lidocaine with epinephrine and injection materials, forceps or lid retractors, straight hemostat, Iris or Stevens scissors.
Technique
The surgical technique for lateral canthotomy is outlined in detail in the procedure page.
Complications
As with any procedure in which tissue is violated, infection and bleeding can occur but are rare, especially with proper technique.
Injury to the corneal in the form of corneal abrasions can occur, especially given the pyroptotic eye. Globe rupture can also occur. Careful lid retraction and instrument handling can help prevent this.
Incomplete or complete loss of normal lid suspension can occur, leading to improper lid positioning, which is a largely cosmetic sequela.[8]
References
[1] Gordon S, Macrae H. Monocular blindness as a complication of the treatment of malar fracture. Plast Reconstr Surg (1946). 1950 Sep;6(3):228-32. doi: 10.1097/00006534-195009000-00005. PMID: 14780862.
[2] Nguyen MV. A Historical Perspective of Lateral Canthotomy and Its Adoption as an Emergency Medicine Procedure. J Emerg Med. 2019 Jan;56(1):46-52. doi: 10.1016/j.jemermed.2018.09.043. Epub 2018 Oct 30. PMID: 30389285.
[3] Gillum WN, Anderson RL. Reversible visual loss in subperiosteal hematoma of the orbit. Ophthalmic Surg. 1981 Mar;12(3):203-9. PMID: 7231876.
[4] https://lovepik.com/download/detail/401795969?byso=&type=0
[5] Shannon B. “Acute Orbital Compartment Syndrome.” https://emedicine.medscape.com/article/799528-overview#showall March 2020.
[6] Oester A, Fowler B, Fleming J. Inferior Orbital Septum Release Compared to Lateral Canthotomy and Cantholysis in the Management of Orbital Compartment Syndrome. Ophthal Plast Reconstr Surg. 2012 Jan; 28(1): 40–43.
[7] McCallum E, Keren S, Lapira M, Norris JH. Orbital Compartment Syndrome: An Update With Review Of The Literature. Clin Ophthalmol. 2019 Nov 7;13:2189-2194. doi: 10.2147/OPTH.S180058. PMID: 31806931; PMCID: PMC6844234.
[8] Desai NM, Shah SU. Lateral Orbital Canthotomy. 2022 Jul 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 32491408.
Your first kit includes specialized materials to practice the Lateral Canthotomy procedure. You may also want to gather materials typically available at home or in your work place. Hang on to your kit pieces, you’ll need them again later.
Estimated Time: 30 Minutes
What’s in the Kit?
- Eye model
- Hemostat
- Iris scissors
- Eye overlay (x3)
What to Bust Back Out
- Tabletop holder
- Suction cups (x4)
Hold onto your kit items, they will need to be reused later!

Ready to jump in?
Click Lateral Canthotomy 1: Procedure Details below to learn about the procedure.