In this podcast we review both boarding and crowding, the twin kiss of death for an Emergency Department, with Dr. Kraftin Schreyer- an Emergency Medicine physician and ED Administrative Fellowship Director. We discuss boarding and how it can be prevented through surge planning, C-suite buy-in, and cooperation between the in-patient and ED. We then go on to talk about crowding and how it is often a kindred spirit of boarding, but can also exist independently. We discuss options for combating this crowding as well.
Practicing procedures can be tough. Let SimKit do all the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. Get 10% off with coupon code SimKit10
Jason Hine: Hello everybody and welcome back to the Simkit podcast. I am joined today by an awesomely special guest. We are happy to be joined by Dr. Kraftin Schreyer who I had the pleasure of calling my co-chief when we were at Temple EM Residency program together. Kraftin is definitely a no-nonsense Workhorse of an ed doc. I think I credit all the knowledge or skills that I have as an em clinician to trying to keep up with her during our training.
She’s an associate professor of emergency medicine at the Lewis Katz school of medicine at Temple University and ED medical director and ED administrative Fellowship director and a medical director of capacity management. a busy individual for sure So Dr. Schreyer, thanks for being on this podcast and tell the listeners a little bit about yourself and what you do now in the world of em.
Kraftin Schreyer: Jay thanks so much for having me. It’s really awesome to have this opportunity to speak with you about operations, which is near and dear to my heart. As you mentioned I’m going to attending Ed physician at Temple and Philadelphia and I currently split my time about 50/50 between clinical shifts and administrative responsibility. I’ve been involved in Ops since residency, and I’ve continued to expand my involvement as my careers progressed. I’ve been a medical director for the past six years and I’ve run our em administrative Fellowship sense Inception in 2018. More recently. I’ve also assumed the role of medical director of capacity management for our health system, which really affords me the unique perspective of looking at operations both from the Ed and inpatient sides.
Jason Hine: Awesome and congratulations on that role in title the medical director of capacity management. Definitely make yeah,…
Kraftin Schreyer: Thank you.
Jason Hine: it makes you the perfect person to talk to today about really probably the bane of every em positions work life. It’s Ed overcrowding and boarding. So I wanted to talk on this topic because really it just doesn’t seem to be getting any better. We’ve all had more patients in your waiting room than beds in your department admit holds in the double digits. If you have a big department triple digits, maybe trying to put portable Telly on your afib rvr patient in the hallway. It is a nightmare. now kraftin there is much to talk about here, but I wanted to keep things tight focused and evidence-based sound, okay?
Kraftin Schreyer: Sure, I mean, I could talk about this all day, but we can keep it tight.
Jason Hine: Keep it to the high yield topics for the Ed physician. So my first question for you is we kind of often marry the two right we marry Edie crowding and…
Kraftin Schreyer: Sounds good.
Jason Hine: We see them as Kindred Spirits. But is there a difference really from an operational standpoint should be we be addressing boarding with a different mind frame than we do edover crowding?
Kraftin Schreyer: So the short answer is from an operational standpoint. There is a difference between crowding and boarding but I’ll say the two are very closely related. Crowding is really defined as when demand ex Supply. So the need for emergency services exceeds the available resources available for patient care, in the hospital or both. Boarding on the other hand is really the extra quote extra time and admitted patient spends in The Joint Commission notes, this is a patient safety risk and says that it shouldn’t exceed four hours, but I’ll say that there really isn’t a shared definition of boarding across emergency medicine. I mean we typically fall back on that joint commission definition of four hours, but maybe that’s not the right number. So boarding, this extra time directly contributes to overcrowding. The longer the patients are holding in the Ed. The fewer beds are available then to see new patients and the more crowding results as new patients present for treatment. I know we all really feel this, like you said kind of more so than ever now, but I’ll say that if anyone’s looking to read some more there was a recent study in Jama from 2022 that did a nice job of quantifying boarding in the context of what we call access block which is also known as Hospital occupancy. So if there are no inpatient beds then Ed patients can’t leave the Ed to go to an inpatient bed.
Kraftin Schreyer: That particular study found that during the pandemic the median Ed boarding time was just over six and a half hours when Hospital occupancy, exceeded 85% compared to just under two and a half hours when Hospital capacity was less than 85 percent which tells you a lot about how the hospitals should operate from a purely flow perspective. yeah so boarding I guess is the primary driver of Ed crowding even though the two are separately defined but to effectively address crowding we have to address boarding.
Jason Hine: That makes sense. You have one kind of leads to the other in its own right? if you Dam up the river, it’s just gonna backflow if people can’t get out. There’s no space to bring people in the boarding leads to crowding. So let’s then talk tackle boarding first. You have a 40-bed Ed on Monday. You come into your five PM Rush with 21 admit holds. Kraftin break down your approach to managing this horrible situation. Let’s talk first about what we can do or what can be done in the department to help.
Kraftin Schreyer: Yeah, unfortunately, not much. I mean if people were looking for quick fixes, I don’t know that I’m going to be able to offer them, in this particular situation. this is really bad, This is the Ed as dangerously overcrowded, on the surface. This looks like a needy problem, but it’s not I think most people listening to this know that it’s really a hospital or health system problem. so, my recommendation would really be for the Ed to push whenever possible and not rely on the floors to pull as an example of an inpatient. If an admitted boarding patient has a ready bed get them out of the Ed, that might mean modifying how your nurse reporters so maybe giving one call attempt before sending the patient up. With some documentation in the rather than waiting for that verbal handoff to happen.
Kraftin Schreyer: Or potentially not relying on third-party transport. So if you have someone in the Ed that you can spare to take the patient upstairs, that might be a good use of that resource. The other solution which I’m sure many listeners have been a part of but is not ideal is getting creative which is seeing new patients in cool non-traditional ways, which might include hallway beds or waiting room medicine which is, not optimal for patient care.
Kraftin Schreyer: A CDs that have search plans that are enacted when the Ed hits critical points of overcrowding. But there’s only so much that can be done within the four walls of the 80 to address this because it really is an external issue. You always have the option of going on EMS diversion, which we’re all familiar with. We know as a patient safety issue and really addresses input which is not the part of Ed throughput where the boarding problem lies. that’s an output access block.
Jason Hine: Yeah, that makes sense. And I like the idea of the push versus pull model, right because part of the challenges are and there might be a different mentality. I don’t know the culture of a lot of inpatient nursing or doc flows. But if we’re busy that usually means they’re busy right once we get over 85% you mentioned we’re gonna start seeing this problem. And so taking on that next patient may not be the high priority option in a nurse that’s approaching sign out. they might hold on that report call for much longer than we want to so the idea of us driving that movement makes a lot of sense to me.
Kraftin Schreyer: Yeah, I think it’s under underutilized. I think you hit the nail on the head, they’re busy but we’re busier I would argue and we have the impetus to prioritize that care for our patients, frankly.
Jason Hine: Yeah.
Jason Hine: Yeah, all right, and then excellent, as you mentioned once the dies kind of cast once you’re at, more than 50% of your beds being occupied by borders, as you mentioned, there’s only so much you can do getting creative rotating people through chairs or triage stretchers to see them put them back in the waiting room get Labs CT scans. What have you will do what we can there and many people are familiar with that. But as you mentioned this is an external issue. So what changes can be made upstairs to deal with this backlog?
Kraftin Schreyer: That’s a great question, in the moment any pending discharger should be reviewed and expedited. that’s kind of a given if your hospital has a discharge Lounge. It should be utilized. I’ll also take the moment to say that a lot of discharge lounges out there have really strict criteria which makes them less useful than they could be. So if you have an opportunity to look at a lounge, I would try to expand it to allow more patients to use it. But anyway, these in the moment actions regarding the discharge patients that are ready to go that day realistically take hours to implement and don’t have the impact we want in the Ed right away. So really you got us think ahead on the inpatient side. You want to avoid that backlog entirely and taking actions, prior to that kind of critical moment. The best practice is really to plan for discharge on the day of admission.
Which a lot of people say they do but don’t actually do there are electronic health records out there that have tools to assist in discharge planning like an estimated date of discharge and discharge Milestones that help identify and anticipate a date of discharge and any potential barriers to actually being discharged on that date, then it allows, some other party to help act on those barriers. Another best practice is early discharges. So getting inpatients out of the hospital before mid-afternoon, when the admissions from the Ed predictably start to increase that will help Continuing dischargers through the weekend in particular helps flow going into a Monday. I mean the scenario you described it’s a typically problematic day for both boarding and crowding so that 24/7 Hospital model over the weekend is really key.
And then lastly I’ll just say that, other actions that can be taken on the inpatient side. You could use impatient hallway beds like we do in the Ed you could also work with your operative services to smooth elective Admissions and operations. All of those have been shown to have positive impacts on Ed boarding and therefore Ed crowding but they’re not common particularly the latter one because there are Financial in implications and anticipated need for increased weekend staff that a lot of Health Systems don’t want to meet the inpatient hallway beds is less common because of pushback from nursing and Regulatory teams, but it has been done. Opening on staff beds, maybe by expanding nursing ratios is also an action that can be helpful for the Ed but also one that’s not easy to implement. And then the final one I’ll say is optimizing turnaround times for EVS and transport helps hospital throughput and therefore Ed throughput
Jason Hine: Yeah, yeah that all makes sense and those structures and systems as you mentioned trying to say, how do we get ourselves out of the hole? We’re in on Monday, at 5 PM, if none of this is in place, you can’t right. Unfortunately all of these take hours days weeks months depending on the Committees involved…
Kraftin Schreyer: Yeah.
Jason Hine: but there are a lot of great practices in there and there are a lot of practices that really should be incorporated into a surge plan that I know our hospital has I believe, Temple system has the same that allow for incremental increases in these areas and it is definitely a culture change and I feel like I’d like to talk a little bit about sort of see sweet or CMO buy-in of if our eating nurses have a ratio of patience and they are just doing everything they can and Staffing well above that. It’s not unreasonable to ask that of our upstairs colleagues or for the
Jason Hine: Mentioned whose bed is being cleaned to be going through intake in that hallway, I do a lot of hospitals want to practice practice continued inpatient hallway medicine. No, it’s not great for patient care. It’s not great for satisfaction scores. But in that time,…
Kraftin Schreyer: Yeah, I mean,…
Jason Hine: that 15 20 minutes between when their room is the patient’s discharged and…
Kraftin Schreyer: I think you bring up a lot of good points there. You certainly need suite buy-in to get a lot of this done and…
Jason Hine: it’s clean for them to enter that opens up space…
Kraftin Schreyer: nursing leader buy-in,…
Jason Hine: where we can do more care in the department.
Kraftin Schreyer: not necessarily nurse managers on the floor…
Jason Hine: Tell me…
Kraftin Schreyer: but like the CNO,…
Jason Hine: if you can any thoughts you have about recognition of buy-in from upstairs.
Kraftin Schreyer: and those direct reports. there’s literature out there that shows that in patients get different care than Ed ICU patients versus observation patients.
Jason Hine: And being a counterpart of ours and really the other half of this problem.
Kraftin Schreyer: So adjusting the ratios. To get the patients where they need to be for the level of care that they need make sense. along that line also take a minute just to tell your listeners to advocate for additional resources for the Ed. So if you’re finding yourself in a place where you’re eating nurses or stretched then maybe your short staff your boarding a bunch of inpatients, sound familiar anyone.
Kraftin Schreyer: You should ask for inpatient nurses to come down and help with those boarding patients, even if there’s no bed upstairs to send them to the level of care that they require is not that that requires me to nurse frankly. So, best practice in my mind would be having the appropriate nurse care for the appropriate patient. So getting those impatient nurses downstairs to care for those cohorted boarded patients would free up your eating nurses to do, Ed care.
Jason Hine:
Kraftin Schreyer: Sorry, I want again.
Kraftin Schreyer: yeah, I mean there’s a good amount of Literature out there like you said on the problems. the one I think that is the easiest read that and as easily translatable when you’re talking to the suite is the Article in the New England Journal by Kellen at all the canary in the coal mine.
Jason Hine: Yep, that’s fantastic. It makes a lot of sense and…
Kraftin Schreyer: We’re probably all familiar with it.
Jason Hine: and we are lucky in our Hospital be able to do that on occasion depending on the number of borders when we hit a certain level.
Kraftin Schreyer: It came out a few years ago. I can send you the actual citation after this J.
Jason Hine: We will try to grab a upstairs nurse to work with a zone of our department.
Kraftin Schreyer: If that would be helpful.
Jason Hine: That’s all admitted patients. and like you said, it involves your CNO getting those people involved one thing. I’d like to ask from you is, references and resources. We have several related to the harms, right? There’s plenty of data about the harms of Ed boarding…
Kraftin Schreyer: Yeah, absolutely.
Jason Hine: but things that people can bring to these sea Suite people or these leaders to sort of show the need and how we all can work cooperatively to make actual gains in terms of patient safety.
Jason Hine: I don’t know if you want to comment on that but basically just references that people can bring to their suite.
Kraftin Schreyer: I think that’s a great question and I’ll put aside the Cost associated with an expansion right the monetary cost the physical plant cost but just speaking if you had a limited resources, if you build it, they’ll come right.
Jason Hine: Yeah, that’d be perfect.
Kraftin Schreyer: Before I get into the expansion answer in detail.
Jason Hine: I think people in the operations world are probably quite familiar with it.
Kraftin Schreyer: I just want to share one piece of key operational thinking that that kind of runs through my mind when I think about Solutions is that every process,…
Jason Hine: But if people are looking to engage themselves in this beyond their throughput committee, their Ed Physicians without that background having that foundational would information be fantastic.
Kraftin Schreyer: every operational process has servers that are required to complete that process. So throughput whether in the Ed or…
Jason Hine: so now I kind of want to talk about…
Kraftin Schreyer: the hospital is contingent on three key servers beds nursing and…
Jason Hine: what intuitively seems like a logical answer…
Kraftin Schreyer: Physicians or…
Jason Hine: but probably may not be Why are we not just making hospitals bigger?
Kraftin Schreyer: One server always serves as a bottleneck in the process. Ideally The Physician is the bottleneck. but more often than not that’s not the case.
Jason Hine: I’ve heard in the prison system for example that they’ve considered building more jails to act to address the prison overcrowding system some have tried it I believe and…
Kraftin Schreyer: So when we’re boarding beds are often that bottleneck or if you’re short staffed on nursing that can be the bottleneck.
Jason Hine: what they find is that when you build more jails you simply end up with a larger scale crowding issue.
Kraftin Schreyer: And as I mentioned neither of those are ideal. We want it to be us. But anyway back to your expansion question, so expanding an ed without any expansion on the inpatient side is not going to fix boarding or crowding. The reason being is in most current admission volume from the Ed exceeds that of the boarding patients.
Jason Hine: so if building more beds is not the solution why is that so
Jason Hine: Yes, millions and millions. Yep.
Kraftin Schreyer: So with more ed beds the additional patients that need to be admitted will be admitted but still have nowhere to go. So you’ll just have more boarding and therefore more crowding. Furthermore you’re gonna have to increase your staff, right? You’ll need both nursing and physician staff to increase to care for these potentially new patients in the additional beds, but when the beds are full of these boarding patients those new staff groups become less productive than originally intended which when you’re talking with a suite and there’s less Roi makes it harder to argue for and maintain that stuff. Building a bigger Hospital on the other hand might solve the problem. It depends a little bit on the admission volume that comes with the Ed and the ignition volume that comes from elective admissions or transfers depending on what type of Hospital you are.
Kraftin Schreyer: But it’s also really dependent on the efficient processes on the inpatient side. So unless they’re is still a focus on early discharging planning early discharges optimal throughput, as I mentioned before these additional beds could just lead to more bed Block. It’s also important to think about what beds you need because the types of beds that are are different. So I see beds or different than men surge beds then surgical beds different than observation beds. So unless you have the appropriately designated beds added to meet the requirements of what your health system needs. Those added beds are going to be for not.
Kraftin Schreyer: That’s right.
Jason Hine: kraftin talk to me about the nedocs score and how if at all we should be using this to assess our Ed situation.
Kraftin Schreyer: So for those who are unfamiliar with it, I call it the nedoc score is one of several measures used to address Ed crowding. It’s a score that was developed back in 2004 It’s calculated from a formula that accounts for the number of patients in The number of hospital beds. The number of ventilators used in the Ed which is kind of a proxy for the ICU admissions. the boarding time for the longest admission the time in the waiting room of the last patient vetted and the number of admissions in the Ed. So any docs calculation generates a crowding score on a scale from 0 to 200 ranging from not busy to Dangerously overcrowded. The scores been studied extensively over the years. I’ll say with mixed results and it unfortunately doesn’t really correlate with provider perception of crowding. And it’s been found to both over and underestimate actual Ed crowding.
Kraftin Schreyer: Plus it’s really complicated to calculate it. I remember when I first got into operations. I tried to do it on shift and even I was struggling to get all the variables. it’s just a lot of information to pull in there. I’ve seen some Ed’s that have it built into the EHR and Incorporated it some way into a hospital surge plan. But I think there are probably other markers of Ed crowding that are more accessible and translatable into Ed and Hospital search plans. maybe Ed occupancy turnaround time, your total Ed volume inclusive of the waiting room. Boarding time or number of borders and you’re left without being seen right? Although I’ll admit that’s a lagging metric So we only feel that after this has become a problem. But any one of those is something that you might be able to use to look at crowding in a way that’s easily communicated to those that need to know.
Jason Hine: Okay, interesting. Yeah, I came across that as part of our operations in admin when we get to our surge capacity red, which is above gray. I guess when we’re gray we’re dead red were still fighting and…we start looking at our needox score and how it flows into our surge plan. So good to know about.
Kraftin Schreyer: Yeah, there are useful scores out there. I’ll say that surge plans. You just reminded me. there are people there that are just living in the red constantly,…if that’s the case, then the search plan isn’t doing… what it’s intended to do. If no action be taken that fixes that problem.
Jason Hine: Yeah, that’s fair.
Transition
Jason Hine: All right. So let’s parcel out our related but sort of possibly separate problem of Ed crowding. Now you may be overcrowded because half of your pay beds are taken by borders, which we kind of talked a little bit about and those situations. We’re looking towards Solutions. We discussed above about sort of throughput and…really an upstairs problem.We have to work cooperatively on that to fix it and we need to be proactive rather than reactive but there are times when emits are kind of moving up freely and : the department still kind of seems to be busting at the seams. What do you do in that situation Krafin?
Kraftin Schreyer: Yeah, I think that’s a great question. it feels like it doesn’t happen frequently, but it still does and…I think this points to the fact that despite, any appropriate push you’d have to have Hospital leadership take a strong stance on the boarding issue. We as the ED still need to take ownership of some parts of Edie crowding that we can control right?
So ED flow, as we think about it is typically broken down into three phases input the in process or throughput piece and then output another things that we can do to address each of these components kind of independent of boarding. so I’ll say, starting with input improving crowding from the input leg is really about reducing demand. So ideally actions would have been taken outside of the Ed to limit demand before it arrives, extending Primary Care hours or having additional Urgent Care is nearby for low Acuity volume. Now, we know that’s not easy for us to do, in a silo but ideally that’s what would happen to reduce demand when the volumes already arrived. There are a few actions you can take to address that access demand.
Kraftin Schreyer: Most commonly people put a provider in triage where the provider evaluates patients upon arrival and then quickly discharges low Acuity patients or potentially orders tests on sick or patients that may need admission or longer Ed care. But I’ll say that that approach. While it does improve your numbers hasn’t been shown to improve throughput and actually can have the opposite impact. Yeah.
But for the next phase the processor throughput piece we can work to improve upon those. This will also require some collaboration this time with ancillary services like lab and Radiology. So acknowledging that we don’t have oversight of those apartments. There are selections the Ed team can take to improve throughput identifying rate limiting results and…
Jason Hine: interesting
Kraftin Schreyer: acting on those in a timely fashion. or using clinical decision rules to limit testing safely and not delay dispositions. And then lastly I’ll mention that, for the output piece aside from admissions, which do account for a lot of Ed output. We can focus on discharge patients. Because improving the discharge turnaround time can only help Ed throughput so specifically optimizing that discharge order to depart time, which may just be a few minutes, right? It might not seem impactful at first is actually A pretty big potential area for improvement if you think about your Ed volume more patients are discharged than admitted. Right? I mean you’re running an admission percentage.
Kraftin Schreyer: Also somewhere between 15 and 25 percent would be my guess, without ever having set foot in your Ed, which means that the rest of the patients right upwards of 70% are discharged. So every minute that you can get back on a discharge patient can be used towards another patient’s care so that time adds up and then suddenly you have this big opportunity cost where you can see additional volume just based on shaving a minute or two off a discharge patients turnaround time here and there.
Jason Hine: No that all makes sense. Perfect.
Alright this has been an awesome discussion about both Edie crowding and boarding and I’m gonna try to do summary crafting and I want you to fill in or you’ll add additional information as I go. How’s that sound?
Kraftin Schreyer: That sounds good.
Jason Hine: Awesome. All right, so we talked about Ed crowding and boarding. We talked about their Kindred Spirits their one often kind of leads to the other right we’re seeing boarding as kind of an upstairs problem or throughput problem and that we need to work with our colleagues to try to decrease our time to admission time to getting the patient out of the department and into the appropriate bed. If we are backing up inboarding then we develop an addressing the boarding element, I really like the idea of the rsus pull model. Of the Ed being in charge of this patient is ready to go upstairs. We are ready to push them up into that space.
And there’s a lot of things that we can do that really are focused on the inpatient side and need to be done in collaboration with our CMO CNL to get these patients up into the space that they deserve that provides higher quality Care Etc. When we’re unable to do that, I do enjoy your commentary on and appreciate it my own practice when upstairs nurses are able to come down and care for Ed patients that are emitted because the quality of care is simply different it’s higher they require a different level of attention and the skills provided by an inpatient nurse are different than those of an eating nurse. we want to advocate for that as well.
When addressing the Ed crowding side, I really liked collectively your idea about servers, and that’s kind of more of a boarding thing. Let me go back to that and then the other thing that I just really liked and want to highlight in terms of the boarding and addressing boarding element are the structuralization or thinking about servers the beds the nursing and Many times the Physicians or the apps are sitting on our hands trying to get to patients in the waiting room and we are not the late rate limiting step when we want to address our boarding issue. We need to look at which of these three servers is the lag and how we can address that and create a surge plan to enact proactively as we get into more crowded circumstances. We will have structuralized surge plans for you that are just sort of templated so that you can bring that back to your department and see how it compares to what you have or what you’re looking to build.
Jason Hine: In terms of the crowding side of things we talked about input processing or throughput and output. When we get into a particularly bad situation where thinking about our time to initiate care, right and a commonly instituted practice is a provider in tree out or the pit doc. I’m surprised and I find it very interesting that this will affect your time to see the physician but maybe not improve any of your other metrics. And Kraftin highlights specifically really trying to Target and be efficient with our time from discharge being ordered being placed in the patient leaving the department because it’s death by a thousand paper cuts or the opposite. I guess of that if you can say five 10 minutes in each discharge patient when you’re discharging, 75% of your patients, you can aggregate a fair bit of time and really improve your efficiency. Kraftin, how’d I do anything, to add to that?
Kraftin Schreyer: I think it did really. I mean this is a complicated topic. There are a lot of moving pieces. Yeah, I think you hit a lot of the details that I would hope people take away from this and I think big picture wise if you’re in the Ed you got to focus on what you can control but it’s also important to optimize your resources collaborate with your hospital or health system leadership. and work to address the boarding and crowding problems. Upstream and early, that’s really the only long-term solution to this. Everything else is kind of a Band-Aid, on a wound that requires much more than that.
Jason Hine: Band aid on a boat hole
Kraftin Schreyer: I was gonna quote Taylor Swift but then I was like no, okay.
Jason Hine: Yeah, you quote T Swift when you want. Yeah, and just to add a final thought on that if this is affecting you were a your quality of work life or your sensation of burnout. Hopefully, there’s some information in here that just is giving you the opportunity to address these issues right to bring this back to your medical director to bring it back to your C suite and say let’s take a look at this see what we have and where we can go from here because it does have a very large impact on the quality of our shifts the quality of care we provide and how we feel as providers.
Kraftin Schreyer: Absolutely I’m a huge proponent of the term I’ve coined “work Wellness.” So if you’re looking to find solutions for your own burnout at work, get involved to find what the problem is and help everyone find a way to fix it and then your life and the lives of everyone you work with is going to be better for it.
Jason Hine: Fantastic, I love Thank you so much, Dr. Schreyer for joining us today, and we hope to have you back on the podcast soon.
Kraftin Schreyer: Yeah, happy to be here. Thanks for having me Jay.
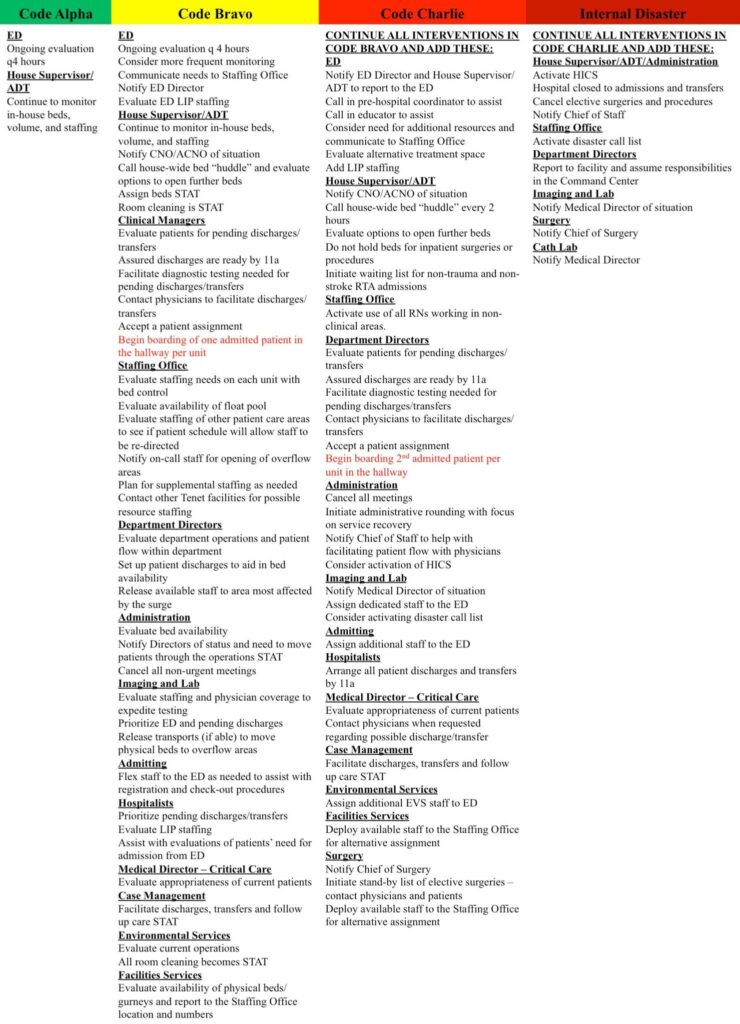
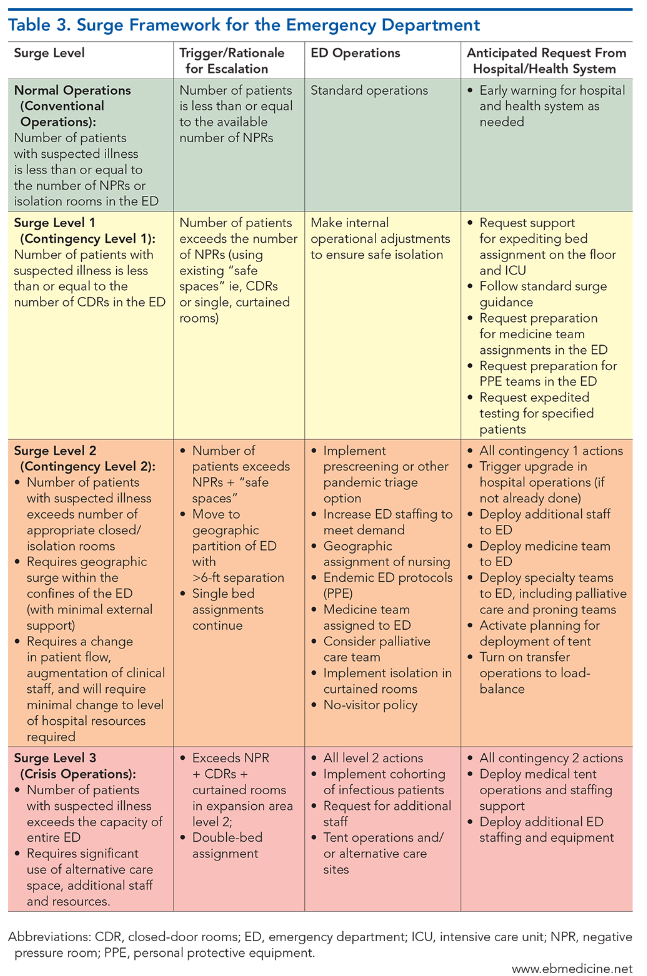
Sample Surge Plan
Having a plan in place for when the Department and Hospital is busting at the seems is invaluable. Below are some sample surge plans. While we cannot recommend adopting these plan wholesale, it is a great starting point for working with your hospital to adjust and adopt a surge plan of your own.
Subscribe to the Podcast on


