Subscribe to the Podcast on



Contact Simkit
Under Pressure
Contributor: Dillon Warr, MD, Jason Hines, MD.
Posterior Reversible Encephalopathy Syndrome (PRES) is a clinical condition that we occasionally encounter in the emergency department and that we should always have on our differential for patients presenting with neurological complaints. In this episode, we break down the pathophysiology, diagnosis, and emergency department management of PRES.
Practicing procedures can be tough. Let SimKit do all the heavy lifting in your skill maintenance. Procedural training can and should be easy, done in your home or department, and work within your schedule. Get 10% off with coupon code SimKit10.
Overview
Posterior Reversible Encephalopathy Syndrome is a clinical radiographic syndrome of multiple etiologies.
It has many names, including Reversible Posterior Leukoencephalopathy Syndrome (RPLS)–though importantly, it is not always reversible nor always in the posterior regions of the brain.
PRES is increasingly recognized, but its pathophysiology is still not fully understood. Proposed mechanisms include disordered cerebral autoregulation, abnormal cerebral vasoconstriction, and endothelial dysfunction
PRES is most commonly associated with hypertensive encephalopathy but also has been described with eclampsia, cytotoxic and immunosuppressant drugs, autoimmune conditions, and kidney disease.
Blood transfusion is another rare cause of PRES that may be under-recognized and has been described in case reports in the neurology literature.
Diagnosis
PRES is a clinical and radiographic diagnosis.
The Clinical Syndrome:
Headache, confusion or decreased level of consciousness, visual changes, and seizures.
All of these components can be quite subtle and require a thorough and detailed history and physical examination.
High blood pressure, although common to many patients with this disease process, is NOT necessary to make the diagnosis.
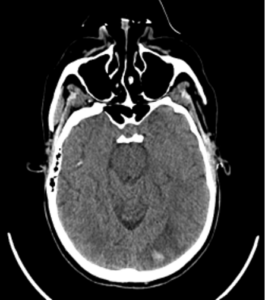
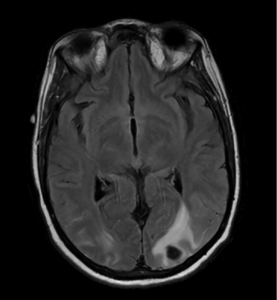
(Typical) Neuroimaging Findings:
Posterior cerebral white matter vasogenic edema.
Intraparenchymal and subarachnoid hemorrhage.
These findings are often apparent on CT (sensitivity ~78%) but are better visualized on MRI (~100%).
Management
Care will include whatever “supportive care” is required in that specific patient case.
The prognosis of PRES is typically favorable if recognized and treated early, with symptom improvement or resolution in a few days to several weeks. But can progress to coma or irreversible ischemia.
Treat seizures if they are readily apparent or you have a high suspicion for seizure activity.
If this patient is pregnant, even if they have radiographic imaging consistent with PRES, call it eclampsia, and treat it as such with magnesium.
There is no specific, established antihypertensive regimen for the treatment of acute hypertension in people with PRES. From the little data that does exist, treatment is recommended if the blood pressure exceeds 160 mmHg/110 mmHg, with a goal of about 130 to 150 mmHg/80 to 100 mmHg. As with our usual treatment for hypertensive encephalopathy, sudden or drastic reduction of blood pressure can lead to cerebral hypoperfusion. Titratable agents such as Clevidipine, Nicardipine, and Labetalol are all great choices.
If this is thought to be due to an immunosuppressive or immunomodulatory medication, stop the med.
Blood Transfusion-Associated PRES
Etiology:
Unclear. Hypothesized that chronic anemia may result in compensatory cerebral vasodilatation. The rapid increase in hemoglobin and viscosity with blood transfusion may cause overwhelming cerebral vasoconstriction or could overwhelm cerebral capillary autoregulation resulting in vasogenic edema and hemorrhage, although these proposed mechanisms are speculative.
Epidemiology:
The available case studies predominantly describe middle-age females with chronic anemia, most commonly caused by menorrhagia, who received large blood transfusion volumes and rapid correction of hemoglobin (an increase in >5 g/dL).
The onset of PRES has been reported to be 1-18 days from the time of transfusion, with a mean onset of ~7 days.
In 75% of cases, the hemoglobin value before blood transfusion was <3.5 g/dL.
Only 38% of these cases presented with hypertension.
Treatment:
Diagnose it and provide supportive care. Treat hypertension if present and manage the seizures.
Prevention:
It may be prudent to limit the initial correction of hemoglobin to <5 g/dL or reduce the rate of transfusion; although, optimal targets are unknown.
References
Referenced Case Report: Warr D, Sammon M, Zhou X, Mullen MT. Case report: Blood-transfusion induced posterior reversible encephalopathy syndrome. Am J Emerg Med. 2024;83:161.e5-161.e7. doi:10.1016/j.ajem.2024.07.026
Other References:
- Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med. 1996;334(8):494-500. doi:10.1056/NEJM199602223340803
- Hefzy HM, Bartynski WS, Boardman JF, Lacomis D. Hemorrhage in posterior reversible encephalopathy syndrome: imaging and clinical features. AJNR Am J Neuroradiol. 2009;30(7):1371-1379. doi:10.3174/ajnr.A1588
- Sudulagunta SR, Sodalagunta MB, Kumbhat M, Settikere Nataraju A. Posterior reversible encephalopathy syndrome(PRES). Oxf Med Case Reports. 2017;2017(4):omx011. Published 2017 Apr 3. doi:10.1093/omcr/omx011
- Dube M, Rathore R. Blood-transfusion-related posterior reversible encephalopathy syndrome – A description of a new case and review of the literature. Brain Circ. 2020;6(4):269-273. Published 2020 Dec 29. doi:10.4103/bc.bc_9_20
- Dou YH, Fuh JL, Chen SP, Wang SJ. Reversible cerebral vasoconstriction syndrome after blood transfusion. Headache. 2014;54(4):736-744. doi:10.1111/head.12319
- Liang H, Xu Z, Zheng Z, Lou H, Yue W. Reversible cerebral vasoconstriction syndrome following red blood cells transfusion: a case series of 7 patients. Orphanet J Rare Dis. 2015;10:47. Published 2015 Apr 22. doi:10.1186/s13023-015-0268-z
- Zhao ZY, He F, Gao PH, Bi JZ. Blood transfusion-related posterior reversible encephalopathy syndrome. J Neurol Sci. 2014;342(1-2):124-126. doi:10.1016/j.jns.2014.05.001
- Wada KI, Kano M, Machida Y, Hattori N, Miwa H. Posterior reversible encephalopathy syndrome induced after blood transfusion for severe anemia. Case Rep Clin Med 2013;2:332.
- Fugate JE, Rabinstein AA. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions [published correction appears in Lancet Neurol. 2015 Sep;14(9):874]. Lancet Neurol. 2015;14(9):914-925. doi:10.1016/S1474-4422(15)00111-8
- Nakamura Y, Sugino M, Tsukahara A, Nakazawa H, Yamamoto N, Arawaka S. Posterior reversible encephalopathy syndrome with extensive cytotoxic edema after blood transfusion: a case report and literature review. BMC Neurol. 2018;18(1):190. Published 2018 Nov 12. doi:10.1186/s12883-018-1194-1